

Translate this page into:
Incidence trends of breast cancer in Saudi Arabia: A joinpoint regression analysis (2004–2016)
⁎Corresponding author. Salbeshan@ksu.edu.sa (Salman M. Albeshan)
-
Received: ,
Accepted: ,
This article was originally published by Elsevier and was migrated to Scientific Scholar after the change of Publisher.
Abstract
Objectives
To report the burden of breast cancer among Saudi females from 2004 to 2016.
Methods
Age-standardised rates and cases according to age, year, region and stage at diagnosis were retrieved from the Saudi Cancer Registry (SCR). Descriptive statistics were reported before joinpoint regression analysis was used to calculate the annual percent change (APC).
Results
During the study period, the number of breast cancer cases increased by 186% from 783 cases in 2004 to 2240 cases in 2016. The median age at diagnosis increased from 47 to 50 years (APC = + 0.7, 95% CI = 0.5 to 0.9) and nearly 60% of cases were diagnosed among women aged ≥40 years. During the study period, the percentage of localised cases increased by 17% (APC = +5.1, 95% CI = 8.7 to 3.3), along with a reduction in regional (APC = −1.3, 95% CI = −0.4 to −4.9) and unknown (APC = −6.5, 95% CI = −12.0 to −0.7) cases. The highest increases in breast cancer cases were recorded in Najran (APC = +8.8, 95% CI = 0.7 to 17.5), followed by Qassim (APC = +6.9, 95% CI = 2.4 to 11.6) and Hail (APC = +6, 95% CI = 3.0 to 9.1). Makkah region reported the lowest significant increase with an APC of +2.3 (95% CI = 0.3 to 4.4) per year.
Conclusion
Although an increasing trend in breast cancer cases were seen over the study period, encouraging outcomes were observed. An incidence shift towards the older age group was noticed, as well as an increased proportion of women diagnosed at early stages. A higher APC was seen in smaller regions, which highlights the need for region-based studies.
Keywords
Incidence
Annual percent change
Breast cancer
Regression
Saudi Arabia

- ASR
-
Age-standardised rate
- SCR
-
Saudi Cancer Registry
- APC
-
Annual percent change
Abbreviations
1 Introduction
Breast neoplasm is the most frequent type of cancer affecting women in Saudi Arabia. In 2018, the age-standardised rates (ASR) for incidence and mortality were 27.3 and 7.5 per 100,000 Saudi women, respectively (IARC, 2020). These rates were found to be lower than those in Western countries such as the United States, where the ASR was 84.9 for incidence and 12.7 for mortality per 100,000 women (IARC, 2020). Previous studies have demonstrated an increasing trend in the incidence of female breast cancer in Saudi Arabia over time (Alghamdi et al., 2013; Althubiti and Eldein, 2018). It was believed that the majority of this increase is, in part, related to the vast socioeconomic shift towards a Western lifestyle—including aspects such as a low prevalence of physical activity, increased consumption of processed food and increased prevalence of tobacco usage—and an aging population (Jazieh et al., 2019; Albeshan et al., 2018).
In a developing country such as Saudi Arabia, where almost 70% of the female population is younger than 39 years (Fig. 1) (SCR, 2016), one of the top priority research areas is to investigate breast cancer characteristics, trends as well as age and geographical variations. The most recent comprehensive epidemiological data on the burden of breast cancer were reported from 2001 to 2008 (Alghamdi et al., 2013), with no up-to-date information readily accessible. We are also not aware whether there have been any changes in breast cancer incidence in terms of region, age group and stage at diagnosis. Therefore, this study was conducted to analyse the burden of breast cancer by exploring the incidence trend and the characteristics of breast cancer for a 13-year period (2004–2016) among the Saudi population using data derived from the Saudi Cancer Registry (SCR). This study also aims to report the distribution of female breast cancer according to year, age, region and stage at diagnosis. Moreover, this study reports the annual percent change (APC) for female breast cancer in Saudi Arabia for each of the administrative regions. This would help policy and health care decision makers to implement prevention and screening strategies as well as allocate resources appropriately.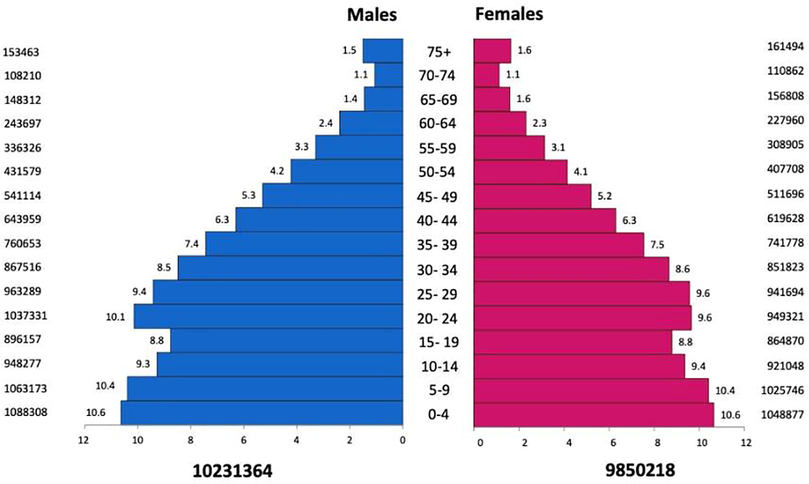
Population pyramids of Saudis according to gender and age group (2016).
2 Materials and methods
2.1 Data source
This study was a retrospective epidemiological analysis of data on Saudi women diagnosed with breast cancer retrieved from the SCR from 2004 to 2016 (NCHI, 2020). The SCR is a certified tumour registry and a publicly available cancer database that collects data from private and government hospitals as well as from laboratories and clinics from all the 13 administrative regions in Saudi Arabia. Cancer information was retrieved from patients’ records based on histopathological and/or clinical diagnosis.
2.2 Statistical analysis
Temporal trends in breast cancer incidence rates according to age group, stage at diagnosis and region were analysed using the joinpoint regression software (NCI, 2020). This analysis involves fitting a series of joined straight lines over successive segments of time on a logarithmic scale. The analysis was performed with the minimum number of join points (a zero join point representing a straight line). The Monte Carlo permutation method was conducted to test at a significance level of 5%. APC was used to describe the direction and magnitude of the resulting trends at a 95% confidence interval (95% CI). This methodology has been used in previous studies to evaluate the changes in breast cancer incidence trends (Baade et al., 2013; Politis et al., 2015; Fares et al., 2019).
3 Results
During the study period, the number of breast cancer cases increased by 186% from 783 cases in 2004 to 2240 cases in 2016. A total of 18,970 breast cancer cases were recorded over the 13-year period (Fig. 2). The ASR increased from 15.4 in 2004 to 27.2 per 100,000 women in 2016 (NCHI, 2020) (Supplementary file 1). This increasing trend was statistically significant at an APC of +3.7 (95% CI = 2.3 to 5.1) per year.
Jointpoint regression analysis of breast cancer incidence in Saudi Arabia (2004–2016). *Indicates that the APC is significantly different from zero at P = 0.05. CI = confidence interval at zero join points. ASR: Age standardised Rate; APC: Annual Percent Change. *Indicates that the APC is significantly different from zero at P = 0.05. CI = confidence interval at zero join points.
3.1 Incidence according to age at diagnosis
The median age at diagnosis was found to increase from 47 years in 2004 to 50 in 2013, 2014 and 2016. This increasing trend was statistically significant at an APC of 0.7 (95% CI = 0.5 to 0.9) per year (Fig. 3). The results showed that almost 60% of breast cancer cases were diagnosed among women aged 40–49 years (31.8%) and among women aged 50–59 years (29.8%, Table 1). For age-specific incidence, the highest APC was seen in women aged 70–74 years (APC = +7.6, 95% CI = 4.7 to 10.7), whereas the lowest was seen in women aged 45–49 years (APC = +2.3, 95% CI = 0.4 to 4.3). ASR: Age standardised rate, APC: annual percentage of change, CI: Confidence Interval.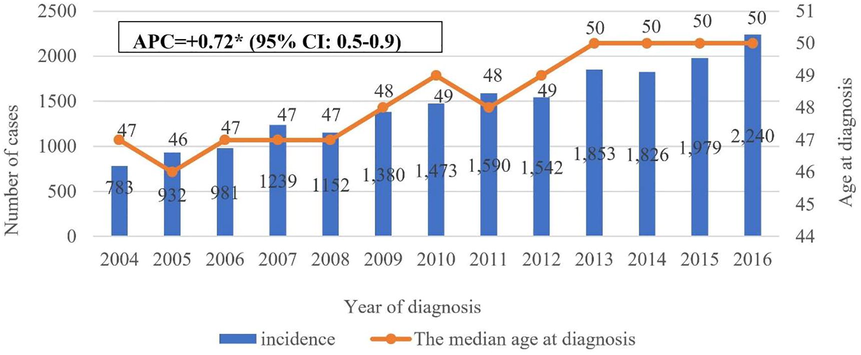
Number of breast cancer cases and median age at diagnosis in Saudi Arabia, 2004–2016. APC: Annual Percentage Change; CI: Confidence Interval. *Indicates that the APC is significantly different from zero at P = 0.05. CI = confidence interval at zero join points.
Age group (years)
ASR (average)
Total number of cases (2004–2016)
APC
95% CI
30–34
13.8
1254
1.6
(-0.6 to 3.8)
35–39
25.8
2050
1.0
(-0.7 to 2.7)
40–44
43.0
2763
1.4
(-0.2 to 3.0)
45–49
61.1
3148
2.3*
(0.4 to 4.3)
50–54
65.6
2712
5.7*
(4.4 to 7.1)
55–59
66.0
2025
4.8*
(2.5 to 7.1)
60–64
64.4
1476
3.5*
(1.1 to 5.9)
65–69
63.3
1033
6.0*
(1.5 to 10.7)
70–74
66.4
801
7.6*
(4.7 to 10.7)
75+
52.8
879
6.3*
(4.6 to 8.1)
3.2 Incidence according to stage at diagnosis
In terms of stage at diagnosis, the percentage of localised breast cancer cases increased from 24% in 2004 to 41% in 2016 (Table 2 and Supplementary file 2). This increase was statistically significant at an APC of +5.1 (95% CI = 8.7 to 3.3) per year. For breast cancer cases reported as regional, although there was a slight decrease from 48.5% in 2004 to 39.7% in 2016, the join point regression analysis indicated that this decrease was statistically significant at an APC of −1.3 (95% CI: −0.4 to −4.9) per year. Furthermore, the findings showed that the proportion of cases with unknown stages decreased from 14% to 7% during the study period (Table 2 and Supplementary file 2). This decrease was statistically significant at an APC of −6.5 (95% CI = −12.0 to −0.7) per year. APC: Annual Percentage Change, CI: Confidence Interval. *Indicates that the APC is significantly different from zero at P = 0.05. CI = confidence interval at zero join points.
Year
Localized (%)
Regional (%)
Distant (%)
Unknown (%)
2004
24
48.5
13.8
13.7
2005
25.4
44.6
12.4
17.5
2006
26.6
45.5
13
14.9
2007
13.7
41.2
12.8
32.3
2008
31.6
42.7
16.2
9.5
2009
31
42.2
18.4
8.4
2010
32.7
39.6
16.9
10.9
2011
31
41
12
16
2012
31.7
42
10
16.3
2013
33
42
13
12
2014
36.1
40
17.3
6.6
2015
38.3
38.6
15
8.2
2016
40.8
39.7
12.5
7
Study period
APC (95% CI)
APC (95% CI)
APC (95% CI)
APC (95% CI)
2004–2016
5.1*(8.7 to 3.3)
−1.3* (-0.4 to −4.9)
0.1(-2.8 to 3.1)
−6.5* (-12.0 to −0.7)
3.3 Regional incidence
The data showed that nearly 70% of the total breast cancer cases were reported in Riyadh (25.2%), followed by Makkah (24.1%) and the eastern region (21.2%). The eastern region recorded the highest average ASR compared with other regions (Table 3). In addition, findings from the joinpoint analysis revealed a statistically significant increase in breast cancer incidence since 2004 in several regions of Saudi Arabia (Table 3 and Supplementary file 2). Of the current trends, the largest significant increase was observed in Najran (APC = +8.8, 95% CI = 0.7 to 17.5), followed by Qassim (APC = +6.9, 95% CI = 2.4 to 11.6) and Hail (APC = +6, 95% CI = 3.0 to 9.1). The Makkah region reported the lowest significant increase, with an APC of +2.3 (95% CI = 0.3 to 4.4). ASR: Age standardised rate, APC: annual percentage change, CI: Confidence Interval. Notes: * Indicates that the APC is significantly different from zero at P = 0.05. CI = confidence interval.
Region
Total number of cases
Average ASR
APC
(95% CI)
Asir
794
10.2
5.7*
(3.6 to 7.9)
Jazan
407
7.8
3.0
(-3.8 to 10.2)
Baha
226
11.5
1.9
(-4.5 to 8.7)
Madinah
1002
16.5
3.4
(-0.2 to 7.1)
Hail
397
14.7
6.0*
(3.0 to 9.1)
Qassim
938
20.2
6.9*
(2.4 to 11.6)
Najran
171
9.6
8.8*
(0.7 to 17.5)
Jouf
289
19.6
4.9*
(0.6 to 9.4)
Tabok
426
17.3
2.5
(-1.5 to 6.7)
Northen
167
14.1
4.4
(-1.0 to 10.1)
Riyadh
4978
27.1
4.6*
(3.0 to 6.1)
Makkah
4567
23.7
2.3*
(0.3 to 4.4)
Eastern
4182
34.0
4.4*
(2.6 to 6.2)
4 Discussion
This epidemiological analysis provides an important information regarding breast cancer with respect to incidence trends, age, stage and the regional distribution in Saudi Arabia. During the study period, the incidence increased almost threefold from 783 cases in 2004 to 2240 cases in 2016. This increasing trend was statistically significant at an APC of +3.7 (95% CI = 2.3 to 5.1) per year (Fig. 2). This rate was close to that reported recently in Lebanon (APC of +4.6% during the period of 2000–2015) (Fares et al., 2019). In comparison, a decreasing trend was reported in New Zealand (APC of −2.2% during the period of 1993–2011) (DeSantis et al., 2015).
The increase in breast cancer incidence in Saudi Arabia can be attributed to a variety of factors, including an aging population (which saw a 50% increase in age from 1999 to 2013) (Bawazir et al., 2019), along with a rapid transition in socioeconomic and traditional lifestyle (Rudat et al., 2012; Bazarbashi et al., 2017). An obvious example of this transition is the increased prevalence of obesity among the female population, a risk factor that is consistently linked to the susceptibility to breast neoplasm (Bazarbashi et al., 2017). A recent study of women undergoing breast screening in Riyadh (N = 744) showed that the majority of these women were classified as overweight (30.1%), obese I (33.6%), obese II (16.1%) or obese III (11.8%). This obesity profile was reported in a large survey conducted by the Ministry of Health (MOH), in which 28% of Saudi women were overweight and 33.5% were obese (Albeshan et al., 2020). Other Western lifestyle-related risk factors for breast cancer, including lack of exercise, an unhealthy diet and the increasing prevalence of smoking and caloric intake, along with genetic predisposition, could be linked to this increasing trend of breast cancer incidence (Althubiti and Eldein, 2018; Jazieh et al., 2019; Albeshan et al., 2018; Bazarbashi et al., 2017).
A previous epidemiological analysis (conducted from 2001 to 2008) showed that the highest incidence of breast cancer cases in Saudi Arabia were reported among women aged 30–44 years (38.6%), followed by women aged 45–59 years (31.2%) (Alghamdi et al., 2013). However, a significant finding of our analysis is an observed slight shift in breast cancer incidence: 43% of cases diagnosed between 2009 and 2016 were among women aged 45–59 years, whereas 30% of cases were reported among women aged 30–44 years.
This slight shift in breast cancer incidence according to age group was reflected in the median age at diagnosis, where there was a 3-year incremental increase from 47 years in 2004 to 50 in 2016. This increasing trend, although small, was statistically significant at an APC of +0.7 (95% CI = 0.5 to 0.9) per year (Fig. 3). This is in contrast with the Western population, wherein women are mostly diagnosed after the age of 50, with a median age of 60 reported among American women, for instance (Albeshan et al., 2020). However, it is a significant finding that the trend in breast cancer incidence among Saudi women is heading in the direction of closing the gap between Saudi Arabian and Western incidence regarding age.
It is well known that Saudi women are more likely to be diagnosed with advanced-stage breast cancer compared with women in Western countries (Albeshan et al., 2020). However, another significate of our analysis is the increased number of localised tumour cases—17%—during the study period (APC = +5.1, 95% CI: 8.7 to 3.3; see Table 2 and Supplementary file 2). This increase in localised breast cancer cases had an impact on the reduction in regional (APC = −1.3, 95% CI = −0.4 to −4.9) and unknown cases (APC = −6.5, 95% CI = −12.0 to −0.7) during the study period. This is likely, in part, related to the early diagnosis through the breast cancer screening program established by MOH that was introduced in 2010. Although a previous study conducted a decade ago reported low screening uptake (El Bcheraoui et al., 2015), there are no recent nationwide data available regarding the participation rate in the screening program (Gosadi, 2019).
In terms of regional incidence, Riyadh, Makkah and the eastern regions have reported the highest number of breast cancer cases (Table 3 and Supplementary file 2). This increase in breast cancer incidence can be explained by the fact that these cities hold most of the Saudi population. For example, Riyadh, as the capital of Saudi Arabia, is home to nearly 22% (7 million people) of the total population (Bawazir et al., 2019). Moreover, this increase is probably also due to the better accessibility of large health centres, particularly those related to the treatment and management of breast cancer (Bawazir et al., 2019).
However, smaller regions, such as Najran, Qassim and Hail (Table 3 and Supplementary file 2), have reported significantly higher APC compared with Riyadh, Makkah and the eastern regions. To explain this variation, in 2004 only 2 cases were reported in Najran, with an ASR of 2.2 per 100, 0000 women. The number increased by 950% to 31 cases in 2016, with an ASR of 17.4 per 100, 0000 women. In comparison, looking to the data from Makkah, one of the highest incidence regions, the number of cases increased from 227 (ASR = 19.1 per 100, 0000 women) in 2004 to 578 in 2016 (ASR = 29.7 per 100, 0000 women) (changes by only 154.6%; please see Supplementary file 1). The increase reported in regional areas such as Najran (APC = +8.8, 95% CI = 0.7 to 17.5) highlights the need for a region-specific epidemiological study that would assist in directing resources towards the most appropriate areas for breast cancer control and management. As breast cancer outcomes are measured by the mortality rate, such a study would be valuable for determining the burden of the disease in Saudi Arabia.
This study has reported the longest analyses of the burden of breast cancer regarding Saudi female. Moreover, no previous research has used the APC for breast cancer-related data including age, stage and regional incidences in Saudi Arabia. However, the limitation of our study is that noted he data regarding the distribution of cases according to age group and stage at diagnosis for each region were not available, which prevented further analysis.
5 Conclusion
The incidence of breast cancer in Saudi Arabia is showing an increasing trend. It was observed that the incidence varied among the administrative regions. However, three encouraging factors concerning breast cancer incidence characteristics among Saudi women were observed. An increasing proportion of cases were diagnosed after age 45 (43%), increasing the median age at diagnosis; likewise, an increase in the number of localised cases (17%) throughout the study period was observed. In general, due to the increasing incidence of breast cancer in Saudi Arabia, it is important to pay more attention to conducting a national, large-scale, region-specific aetiological risk factor study. Such a study would subsequently be helpful in directing resources towards the appropriate areas for breast cancer control and management.
Declaration of Competing Interest
The authors declare that they have no known competing financial interests or personal relationships that could have appeared to influence the work reported in this paper.
References
- Breast cancer epidemiology in gulf cooperation council countries: a regional and international comparison. Clin. Breast Cancer. 2018;18(3):e381-e392.
- [CrossRef] [Google Scholar]
- Can Breast self-examination and clinical breast examination along with increasing breast awareness facilitate earlier detection of breast cancer in populations with advanced stages at diagnosis? Clin. Breast Cancer. 2020;20(3):194-200.
- [CrossRef] [Google Scholar]
- Alghamdi, I.G., Hussain, I.I., Alghamdi, M.S., El-Sheemy, M.A., 2013. The incidence rate of female breast cancer in Saudi Arabia: an observational descriptive epidemiological analysis of data from Saudi Cancer Registry 2001–2008. Breast Cancer. 5,103−109.
- Trends in the incidence and mortality of cancer in Saudi Arabia. Saudi Med. J.. 2018;39:1259-1262. doi: 10.15537%2Fsmj.2018.12.23348
- [Google Scholar]
- Epidemiology of prostate cancer in the Asia-Pacific region. Prostate Int.. 2013;1:47-58.
- [CrossRef] [Google Scholar]
- The burden of leukemia in the Kingdom of Saudi Arabia: 15 years period (1999–2013) BMC Cancer. 2019;19:703.
- [CrossRef] [Google Scholar]
- Cancer incidence in Saudi Arabia: 2012 data from the Saudi cancer registry. Asian Pac. J. Cancer. Prev.. 2017;18:2437. doi: 10.22034%2FAPJCP.2017.18.9.2437
- [Google Scholar]
- International variation in female breast cancer incidence and mortality rates. Cancer Epidemiol. Prev. Biomark.. 2015;24(10):1495-1506.
- [CrossRef] [Google Scholar]
- Breast cancer screening in Saudi Arabia: free but almost no takers. Plos One.. 2015;10(3):e0119051.
- [CrossRef] [Google Scholar]
- Breast cancer epidemiology among Lebanese women: an 11-year analysis. Medicina.. 2019;55:463.
- [CrossRef] [Google Scholar]
- National screening programs in Saudi Arabia: Overview, outcomes, and effectiveness. J. Infect. Public Health.. 2019;12(5):608-614.
- [CrossRef] [Google Scholar]
- International Agency for Research on Cancer. The Global Cancer Observatory (GCO), Available at: https://gco.iarc.fr. Accessed: October 11, 2020.
- Jazieh, A.R., Da’ar, O.B., Alkaiyat, M., Zaatreh, Y.A., Saad, A.A., Bustami, R., Alrujaib, M., Alkattan, K., 2019. Cancer incidence trends from 1999 to 2015 and contributions of various cancer types to the overall burden: Projections to 2030 and extrapolation of economic burden in Saudi Arabia. Cancer Manag. Res. 11, 9665−9674. doi: 10.2147%2FCMAR.S222667.
- Kingdom of Saudi Arabia Council of Health Services, Saudi Cancer Registry (SCR). Cancer Incidence Report: Saudi Arabia 2016, Available at: https://nhic.gov.sa/en/Pages/default.aspx. Accessed: July 25, 2015.
- National Cancer Institute (NCI), Division of cancer control and population sciences. Available at: https://surveillance.cancer.gov/joinpoint/. Accessed: August 8, 2020.
- National Centre for health information. Available at: https://nhic.gov.sa/en/Pages/default.aspx. Accessed: August 8, 2020.
- Trend analysis of cancer mortality and incidence in Panama, using joinpoint regression analysis. Medicine.. 2015;94:970. doi: 10.1097%2FMD.0000000000000970
- [Google Scholar]
- Epidemiology of breast cancer patients at a tertiary care center in the Eastern Province of Saudi Arabia. Gulf J. Oncol.. 2012;1:45-49.
- [Google Scholar]
Appendix A
Supplementary data
Supplementary data to this article can be found online at https://doi.org/10.1016/j.jksus.2021.101578.
Appendix A
Supplementary data
The following are the Supplementary data to this article:




