

Translate this page into:
Cohort study on the food safety knowledge among food services employees in Saudi Arabia state hospitals
⁎Corresponding author. alialrasheed1403@gmail.com (Ali Alrasheed) alfalrasheed@moh.gov.sa (Ali Alrasheed)
-
Received: ,
Accepted: ,
This article was originally published by Elsevier and was migrated to Scientific Scholar after the change of Publisher.
Peer review under responsibility of King Saud University.
Abstract
Hospital food safety is of paramount importance as patients are vulnerable to acquired diseases transmitted by unsafe food. The focus of this research was to critically analyze food safety and hygiene knowledge in Kingdom of Saudi Arabia (KSA) in respect of compliance with Hazard Analysis and Critical Control Points (HACCP) and International Organization for Standardization (ISO22000). Interviews of 242 randomly selected food services employees from seven KSA hospitals were carried out. Roles ranged from catering workers and catering supervisors together with Ministry of Health (MOH) supervisors. The survey was designed to evaluate their level of education, training, ethnicity, level of understanding and knowledge of food safety management systems, such as HACCP. Amongst an ethnically diverse group of catering workers, education levels were adequate but hygiene training in some of the hospitals investigated could be improved and the training should start immediately upon employment. The group of catering supervisors were well-educated but the survey identified some weaknesses in their knowledge and understanding of HACCP. The MOH supervisors group were all Saudi nationals and also showed some weakness in their knowledge and understanding of HACCP. The food policies in KSA need to be more accessible to their target audience and the format of the policies would benefit from increased consultation at all levels of the food supply chains.
Keywords
Food safety policies
HACCP
ISO22000
Hospitals
Saudi Arabia

1 Introduction
The food chain extends from production on farms, through processing, shippering, retail, food preparation, to eventual ingestion by consumers. Challenges in this process include: microbial, chemical, physical, personal and environmental hygiene (Al-Ghazali et al., 2020). Food is essential to life but billions in the world are at risk of unsafe food. Many millions become sick while hundreds of thousand die yearly (Fung et al., 2018). Centers for Disease Control and Prevention (CDC) in 2017 reported that every year around 50 million people suffer from food-related infections leading to about 3000 mortalities (WHO, 2017). Hazard Analysis and Critical Control Points (HACCP) is a systematic preventive approach to food safety that aims to reduce the risk of biological, chemical and physical hazards in food production (Schmidt et al., 2003). It can be applied to all stages of a food chain, such as food production, preparation, packaging and distribution. Although HACCP applies to all food businesses, it is of particular importance to hospitals where patients are more vulnerable and therefore more susceptible to microbial contamination (Heever et al, 2016). The problems hospitals face implementing these procedures are similar to the problems faced by other food businesses, such as lack of financial support, absence of training programmes (Khatri and Collins, 2007), and inadequate eqnuipment to perform their job to the best of their abilities (Garayoa et al, 2011). Hospitals have the additional problem of stocking a broad and diverse range of products, all of which require specific processes and usages, this can potentially limit HACCP implementation (Williams and Wallace, 2001).
Safety of the healthcare-based food is a major challenge in the hospital facilities. Implementation of proper food preparation and handling practices for the food handlers in the healthcare facilities is of paramount importance in protecting the well being of the patients and hospital staff (Alqurashi et al., 2019). Recently, global research has focused on the knowledge, attitudes and self-reported practices of the food handlers on food safety. Although self-reported practices may not be the actually practiced behavior, as the respondent may have been biased while reporting (Ncube et al., 2020).
In Kingdom of Saudi Arabia (KSA), matters related to food safety and hygiene are covered by Ministry of Health and Saudi Food and Drug Authority (SFDA). National legislation in Saudi Arabia requires food safety to be managed using a documented, HACCP based approach. This requires all food handlers to be appropriately trained in food safety (Walker et al., 2003). The SFDA was established to apply food hygiene requirements in all food operations. This is monitored by Saudi Food Inspectors (SFIs) who perform a similar role to Environmental Health Officers in the UK or Food Safety and Inspection Service (FSIS) Officers in USA, in that they are responsible for inspecting businesses that produce food and ensuring that these businesses conform to accepted standards. However, Al-Mutairi (2013) found in his observation of SFIs, that serious breaches of ISO 22000 or HACCP can be overlooked in spite of the majority of inspectors having good quality training in the food hygiene practices. Such inconsistencies may explain why food businesses have little faith in food safety regulations, as was concluded in an empirical study carried out by Wilson (2015).
The MOH in Saudi Arabia is in charge of the implementation of the HACCP procedures in all state hospitals food services. The MOH was mandated responsibility for the supervisory role for food preparation as well as nutrition in Saudi hospitals in 1981, whereby they issued a contract which contains guidelines for state hospitals, called the Nutrition Service Programme for State Hospitals (MOH-KSA). In 2010, MOH hospitals served 19.2 million meals with an average of 53,952 daily meals, this included breakfast, lunch and dinner (MOH-KSA, 2020). There are currently 25 Saudi based foodservice companies in Saudi Arabia that specialise in healthcare catering. These companies are selected via a tendering process. Suitably educated staff for the specific roles are recruited from around the world. Qualifications are checked by the Nutrition Department prior to work commencing. Catering staff are also expected to successfully renew health licenses every six months. The health license validates that the employee is free from any infectious diseases. Failure to comply with contractual agreements can result in a variety of sanctions and penalties, depending on the violation. Contracts run for a specified time, usually three years, so that the process and working conditions can be frequently reviewed to ensure all parties are satisfied with the arrangement and that MOH conditions have been adhered to (MOH-KSA, 2020).
To further improve food standards, contracts now require caterers to implement HACCP in hospitals kitchens. These are overseen by the KSA MOH hospital nutrition management team. In 1994, the HACCP Alliance was formed to ensure standards are met and implemented. The HACCP system is guided by seven basic principles which must be considered in any premises where food is produced. Notwithstanding the fact that Saudi Arabia's MOH plans to introduce HACCP in all hospitals, there has not yet been serious consideration given regarding the readiness of hospitals, be they small (50–100 beds) or medium (150–350 beds), to make such a system work (MOH-KSA, 2020).
The role of MOH Supervisors is to evaluate the patients’ nutrition while they are in hospitals and adjust and improve this where needed, in line with individual needs and nutritional guidelines (MOH-KSA, 2020). MOH supervisors must work in compliance with regulations outlined by the General Directorate of Nutrition, which regulate processes at state hospitals. Their role is to raise awareness of recent regulations and disseminate this to catering supervisors. MOH supervisors have ultimate responsibility for food safety in state hospitals as they award the catering team contracts. Therefore, MOH Supervisors must be suitably trained and fully aware of all legislation (MOH-KSA, 2020). KSA state hospitals rely on HACCP and the Ministry of Health document called Food Services Contract; however, the information needs to be broken down into a more user-friendly format. In order to do this it is important to determine where strengths and weaknesses lie. This can be achieved by an anonymous survey staff at each level. A new policy must be designed to address roles and responsibilities of all staff, as well as specific instructions on the monitoring of all relevant processes related to food safety.
This research may be used as a model for more structured transfer of good practice from a developed country to developing and under-developed countries to reduce the time necessary for HACCP and ISO 22000 to become recognised and applicable. The survey aimed to test food safety and hygiene policy knowledge; self-monitoring and attitudes of food handlers and also address data deficiencies such as the lack of demographic data relating to age, sex, education level, ethnicity and nationality of hospital staff in Saudi Arabia.
2 Materials and methods
2.1 Participating hospitals
The primary research was conducted in seven KSA state hospitals namely KFMC, KSMC, KSH, AAA, ALIMH, ALYMH and PMPA hospital from September 2018 to May 2019.
2.2 Data collected
The research methodology included the analysis of primary data obtained from KSA state hospitals on the issues related to food safety and hygiene policies and specification or guidelines. Also, the study analysed how HACCP was being implemented in nutrition departments, especially among food supervisors and managers. An audit was used to assess the status of the hospital prior to implementation of the HACCP system. An analysis of the policies was undertaken to determine if there was any standardization in approach to food safety, structure of organization and delegation of duties, monitoring and regulatory practices.
2.3 Survey design
Questionnaire (A, B and C) was designed as described previously (Al-Shabib et al., 2015).
Questionnaire A was specifically for those who handle food such as butchers, chefs and their assistants, waitresses and waiters, and stores workers among others. The questions related to knowledge looked at cross contamination, microbiology, and temperature control, and the effect of the training program. There were 22 questions asked in total to this group.
Questionnaires B and C were designed for staff employed by catering companies and MOH. There were 25 questions asked in total to groups B and C. The questions asked for information about demographics, attitudes, practices, and knowledge. Poisoning, microbiology, hygiene practices, and food safety management.
Three hundred and twenty-nine subjects were randomly selected. A cover note was provided written in Arabic and English that explained the objectives of this study. Participation was purely voluntary and participants were free to withdraw at any point (according to School of Sociology & Social Policy, Research Ethics Checklist for Students and Staff). A total of 242 completed forms were returned.
2.4 Statistical analysis
The data management and analysis were performed using Software for Statistics and Data Science (STATA). Statistical significance was determined using P < 0.05. A null hypothesis attempts to demonstrate that between variables there is no variation or that a variable is not different from its mean. If p- value is <0.05 then the null hypothesis is rejected, and the alternative hypothesis will be acknowledged. In other words, rejection of the null hypothesis “p < 0.05“ shows that a significant difference exists, and the result is significant.
3 Results
3.1 Education level of survey group
The survey included data from 242 (41.3% male and 57.8% female), randomly selected food services employees from seven KSA hospitals. Contracted catering workers (148 respondents), hospital catering Minsitry of Health supervisor (MOH) supervisors (80 respondents), and the catering supervisors employed by the contracted catering companies (14 respondents). The level of education was generally high and appropriate for each of the three main role groups (MOH supervisor, contracted catering supervisors and contracted catering workers; Fig. 1A). Amongst the contracted catering workers, the education levels was analysed further from each individual hospital. The most suitably qualified catering workers were employed at AAA with 73% of catering workers holding a Diploma and 9% with a Bachelor qualification. ALIMH hospital had a high proportion of qualified catering workers with 15% Bachelors and 62% Diplomas. Only 3% of the catering workers at this hospital had basic food hygiene qualifications. PMAH employed 50% of catering workers with Bachelor degrees and 28% with Diplomas (Fig. 1B). This clearly dispels any assumption that catering workers are unqualified.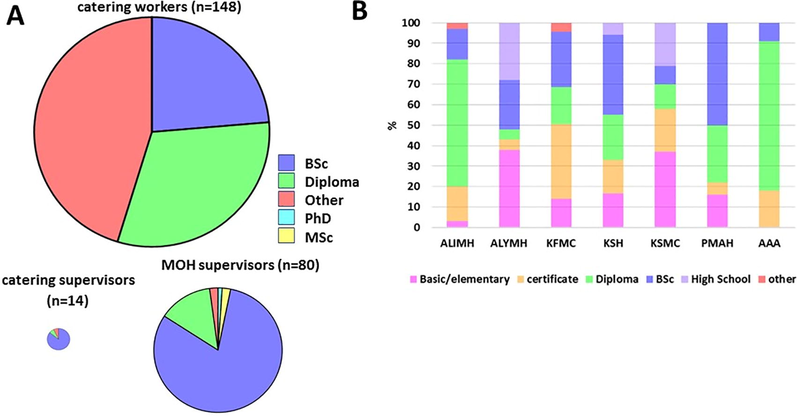
Education levels of workers included in the survey. A) comparison of the three groups. B) Education levels of catering workers from each hospital.
3.2 Ethnicity
The survey collected information on the ethinicity of the workers employed in the different roles, which is summarized in Fig. 2. The survey revealed that 76% of the catering workers were non-Saudi nationals, predominantly drawn from the Philippines and India. In contrast, all MOH supervisors were Saudi nationals. The contract catering supervisors were Saudi (36%), Egyptian (43%) or Indian (21%) nationals.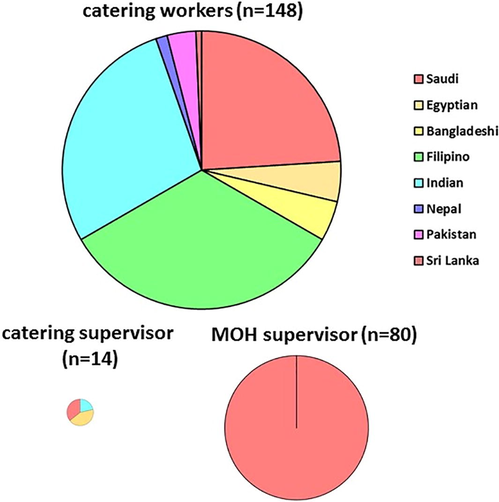
Ethnicity of the survey groups.
3.3 Hygiene training for contracted catering workers
Contracted catering workers were questioned as to whether they had received basic hygiene training (Fig. 3). The results showed considerable variation between the seven hospitals. KSMC and KFMC hospitals scored highly, with almost all catering workers reporting that they had received basic training. However, the answer to this question were a cause for concern at the other five hosptials. The difference of having any hygiene training or not between the hospitals was statistically significant (P = 0.001). However there was no significant correlation between hygiene training and any demographic characteristic such as gender, nationality, salary or qualification (P value >0.05). The only parameter that had a statistically significant correlation was the employment length where the P value was 0.04 using an independent t-test. The results showed that workers who had hygiene training had a mean length of employment of almost three years (35.8 months) and a median of 24 months. Workers who had not received any hygiene training had a mean length of employment of less than two years (23.8 months) and a median of 12 months.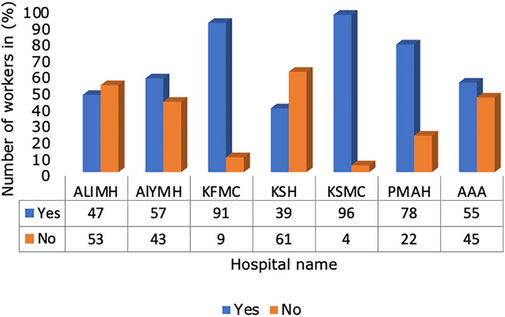
Hygiene training for contracted catering workers.
3.4 Catering workers reporting procedures in case of illness
The majority of workers in six of the seven hospitals understood the need for basic reporting procedures when they were sick or vomiting to ensure that this illness is not spread to other people (Fig. 4). They were aware that they need to visit their GP to confirm the illness, and then inform their manager about the reason for their absence. Of these, only KSMC gave a 100% response that they should inform their line manager. However, a high proportion of staff at AAA (91%) answered that they would visit the GP out of hours and 9% answered that they will go to work as usual and not inform superiors so as to avoid being unpaid for that day. This suggests that that they had not been made fully aware of the importance of personal health and hygiene, and the consequent effect this may have on patients. They also felt that being absent from work was only possible once the results of the illness were confirmed. This is a risk to health as it means they would continue to work while potentially being ill and posing a risk to the patients. Ensuring that staff are aware of their responsibilities to patients and that it is acceptable to miss work on such occasions is something that needs to be addressed through proper training of both line managers, who enforce the rules and safeguard patients, and the staff affected by the illness. Two hospitals, ALYMH (14%) and KSH (6%), had a low percentage of workers who stated they were unsure what to do. Even though this percentage is small it is something that needs to be addressed to ensure standardised procedures are in place. KSH also had the highest proportion of workers (28%) who said they would still go to work and not inform their line manager through fear of not being paid. This suggests that management need to make it clear that it is acceptable to miss work due to hygiene issues that could affect patients. The correlation of differences between hospitals in terms of sickness procedure was statistically significant (P = 0.001) while it was not statistically significant with any of the demographics. Moreover, workers who had hygiene training were more likely to answer this question correctly than workers who did not attend any hygiene training (P = 0.05). This means that they understood the correct procedure for dealing with illness during the training programme.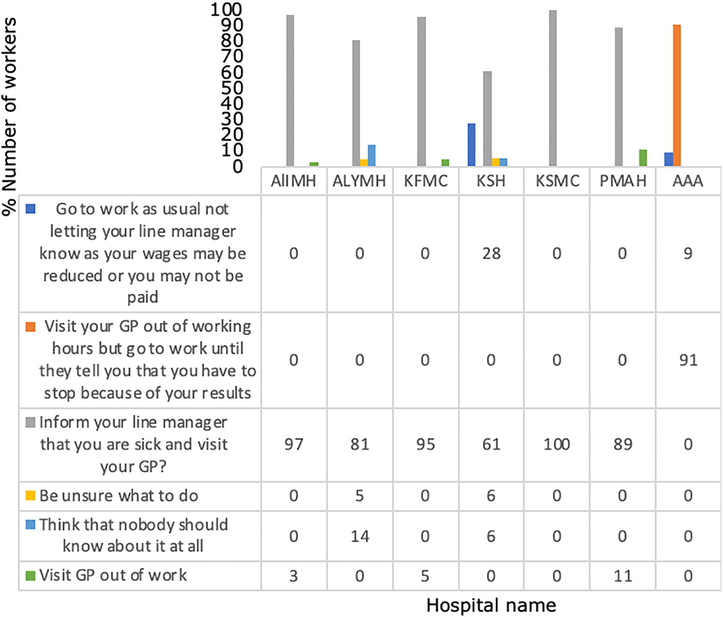
Reporting procedures of catering in case of illness.
3.5 Monitoring procedures for HACCP by contract catering supervisors and MOH supervisors
The fourteen contract catering supervisors were questioned about HACCP Principle 4 monitoring procedures (Fig. 5). Nine contracted catering supervisors provided the correct answer ‘All of the above’. However, the remaining five supervisors provided inadequate answers. In three hospitals the supervisors believed that monitoring was specific to refrigerators, whereas the contracted supervisors at the other two hospitals thought that monitoring only involved critical control points. When this data is broken down into demographics the results show that young and less experienced overseas supervisors, and dieticians with Saudi qualifications, all exhibited incomplete knowledge and require further training in this area. However, not all experienced supervisors provided the correct answer, suggesting that experience without continuous training cannot be relied on. The responses selected by the contracted managers from different hospitals were not significantly different (P = 0.28). Inappropriate answers could not be correlated with any specific demographic.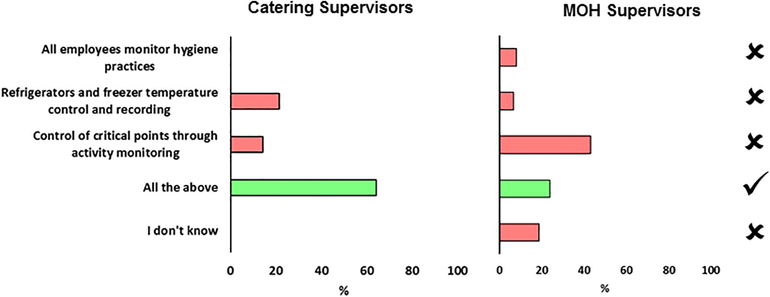
Level of HACCP monitoring procedures among contract catering supervisors and MOH supervisors.
The same question was put to the 80 MOH supervisors (Fig. 5) in relation to monitoring procedures for HACCP Principle 4. It is interesting to note that at KSH 85% of supervisors thought that control of critical points through activity monitoring was sufficient. More worryingly, there were five hospitals who respondents indicated that they did not know the answer. These were: KSH (15%) PMBA (9%) ALYMH (29%) ALIMH (14%) and AAA (64%). Similarly, a wide variety of possible answers were provided, suggesting specific training is required in the area of HACCP monitoring procedures in Riyadh’s state hospitals. All these responses were correlated with the distribution across hospitals. The only demographic group that correlated with inappropriate answers was the qualification parameter. Of those who were holding diplomas, 55% answered incorrectly, which was significant (P = 0.012).
4 Discussion
The MOH, KSA regulations, stated that, food catering services at hospitals, should comply with HACCP and ISO22000 as part of the Nutrition Services Programme for KSA State hospitals. Saudi Hospitals involved in this study (seven KSA hospitals), all were applying HACCP and ISO22000. One of the measures to control food safety is applying roles and guidelines of food safety to minimize, or eliminate a potential food safety hazard from occurring (Boqvist et al., 2018). In this study, all contract catering supervisors were aware of the purpose of HACCP (Fig. 5). Whether only three out of seven of the MOH supervisors gave the correct answer and were unsure about purpose of HACCP. Identifying and implementing adequate control measures is an important for food business producing safe food (Boqvist et al., 2018). Food handlers, involved in preparing and serving food, working with poor personal hygiene could pose a potential threat of spreading intestinal parasites to the public in a community, which may be a risk for transmitting intestinal parasites to food and drinks consumers through the food chain (Yimam et al., 2020).
In this study, the level of education was generally high and appropriate for each of the three main role groups (MOH supervisor, contracted catering supervisors and contracted catering workers as illustrated in (Fig. 1A). A Brazilian food handlers' knowledge and practices study, illustrated that, an average of 72.64% of food safety knowledge were correct answers. Food safety self-reported practices presented 80.71% of adequacy, while observed practices were 75.40%. A positive correlation has been observed between food safety knowledge and self-reported practices of handlers (de Souza et al., 2018).
In the current investigation, both KSMC and KFMC hospitals, almost all catering workers reported that they had received basic training. In the other five hospitals, training for only some of them, especially those who had a mean length of employment of almost three years (Fig. 3). Akabanda and his colleagues reported that, food-handlers were aware of the critical role of general sanitary practices in the work place, such as hand washing (98.7% correct answers), using gloves (77.9%), proper cleaning of the instruments/utensils (86.4%) and detergent use (72.8%) (Akabanda et al., 2017). In this study, there was no significant correlation between hygiene training and any demographic characteristic such as gender, nationality, salary or qualification.
Further, education levels amongst the 148 contracted catering workers were analyzed from each individual hospital (Fig. 1B). Increased knowledge was consistently associated with safe food handling behaviors (Young et al., 2019). This clearly dispels any assumption that catering workers are unqualified. The survey revealed that 76% of the catering workers were non-Saudi nationals, predominantly drawn from the Philippines and India (Fig. 3). All MOH supervisors were Saudi nationals (Fig. 3).
Akabanda and his colleagues reported that food-handlers were aware of the critical role of general sanitary practices in the work place, such as hand washing (98.7% correct answers), using gloves (77.9%), proper cleaning of the instruments/utensils (86.4%) and detergent use (72.8%) (Akabanda et al., 2017).
A study from Africa, showed 76.2% of the food- handlers did not know that Salmonella is a food borne pathogens and 81.7% handlers agreed that typhoid fever is transmitted by contaminated food (Akabanda et al., 2017). In this study, the majority of workers in six of the seven hospitals understood the need for basic reporting procedures when they were sick or vomiting to ensure that this illness is not spread to other people (Fig. 4). This is in agreement with the report published on the knowledge and practices of food handlers employed in university restaurants (Al-Shabib et al., 2015). In another study, wide variety of predictive power in the behavior of food handlers was reported (Young et al., 2018). This may suggests that they had not been made fully aware of the consequent effect that this may have on patients, such as continue to working while potentially being ill and posing a risk to the patients. Food handlers may be asymptomatic carriers of food poisoning organisms and serving as a potential source of contamination to food (Roberts et al., 2008, Cruickshank, 1990). Adequate training can help limit food contamination and reduce the resulting effects of contamination on health and economy food (Roberts et al., 2008).
Ensuring that staff are aware of their responsibilities to patients and that it is acceptable to miss work on such occasions is something that needs to be addressed through proper training of both line managers, who enforce the rules and safeguard patients, and the staff affected by the illness. In this study two hospitals, ALYMH (14%) and KSH (6%), had a low percentage of workers who stated they were unsure what to do. Even though this percentage is small it is something that needs to be addressed to ensure standardised procedures are in place. KSH also had the highest proportion of workers (28%) who said they would still go to work and not inform their line manager through fear of not being paid. In a study conducted on 138 food handlers, 2.26 (95% CI: 1.57, 3.25) did not take up medical checkup, and 1.79 (95% CI: 1.30, 2.45) did not receive food safety training (Alemnew et al., 2020).
This suggests that management needs to make it clear that it is acceptable to miss work due to hygiene issues that could affect patients. The correlation of differences between hospitals in terms of sickness procedure was statistically significant (p = 0.001) while it was not statistically significant with any of the demographics. Moreover, workers who had hygiene training were more likely to answer this question correctly than workers who did not attend any hygiene training (p = 0.05). This means that they understood the correct procedure for dealing with illness during the training programme. Food handlers may be infected by a wide range of enteropathogens and have been implicated in the transmission of many infections to the public (Alemnew et al., 2020).
5 Conclusion
The main findings of this research reinforce the importance of training and the need to develop food policies for hospitals that ascribe ways of working that are underpinned by level specific training. These intiatives lead to general implementation of food safety standards commensurate with providing meals for vulnerable hospital patients. Although KSA is committed to improving food safety standards by the implementation of international standards represented by HACCP and ISO22000. Ministry of Health needs parallel developments in hospital policies, such as Food safety and hygiene policies to establish standardised operations, which will outline best practices and at the same time may still permit some individual differences based on the specific contexts in which the policies are enacted. One more aspect of particular importance is the standardised introduction of processes by appropriate level-specifc training. This research highlights the importance of the need to regularly assess food safety operations and management, and to ensure the policies adopted are implemented. On the contrary, one limitation of the current study could be the substantial discrepancies between self‐reported and observed food handling practices, self‐reports underestimate the magnitude of undesirable food handling practices. This highlights the need for future food safety studies to use observation to validate food handlers’ self‐reports about their food handling practices.
Acknowledgements
The authors would like to extend their sincere appreciation to the ‘Researchers Supporting Project’ number (RSP-2021/84), King Saud University, Riyadh, Saudi Arabia.
Declaration of Competing Interest
The authors declare that they have no known competing financial interests or personal relationships that could have appeared to influence the work reported in this paper.
References
- Food safety knowledge, attitudes and practices of institutional food-handlers in Ghana. BMC Public Health. 2017;17(1):40.
- [CrossRef] [Google Scholar]
- Prevalence and factors associated with intestinal parasitic infections among food handlers working at higher public University student’s cafeterias and public food establishments in Ethiopia: a systematic review and meta-analysis. BMC Infectious Dis.. 2020;20(1):156.
- [CrossRef] [Google Scholar]
- Food safety knowledge and hygienic practices among different groups of restaurants in Muscat, Oman. Int. J. Food Sci.. 2020;2020:1-8.
- [CrossRef] [Google Scholar]
- UK: University of Nottingham; 2013. PhD thesis
- Evaluating food safety knowledge and practices among foodservice staff in Al Madinah Hospitals, Saudi Arabia. Safety. 2019;5:1-16.
- [CrossRef] [Google Scholar]
- Cross-sectional study on food safety knowledge, attitude and practices of male food handlers employed in restaurants of King Saud University, Saudi Arabia. Food Control. 2015;59
- [CrossRef] [Google Scholar]
- Food safety challenges and One Health within Europe. Acta Veterinaria Scandinavica. 2018;60(1):1.
- [CrossRef] [Google Scholar]
- Food safety in Brazilian popular public restaurants: Food handlers’ knowledge and practices. J. Food Safety. 2018;38(5)
- [CrossRef] [Google Scholar]
- Garayoa et al., 2011. Food safety and the contract catering companies: Food handlers, facilities and HACCP evaluation. Food Control 22, 2006–2012. 10.1016/j.foodcont.2011.05.021.
- Heever et al, 2016. Microbial contamination and labelling of self-prepared, multi-dose phenylephrine solutions used at a teaching hospital. South. African J. Anaesth. Analg. 10.1080/22201181.2016.1251062.
- Impact and status of HACCP in the Australian meat industry. British Food J.. 2007;109(5):343-354.
- [CrossRef] [Google Scholar]
- Ministry of Health Portal, Saudi Arabia (2020). Available online: http://www.moh.gov.sa/en/Ministry/Pages/default.aspx.
- Ncube, F., Kanda, A., Chijokwe, M., Mabaya, G., Nyamugure, T., 2020. Food safety knowledge, attitudes and practices of restaurant food handlers in a lower‐middle‐income country. Food Sci. Nutr. 8, 1677–1687. 10.1002/fsn3.1454.
- Food safety training and foodservice employees. Food Safey Train. Foodservice Employees. 2008;28(4):252-260.
- [Google Scholar]
- Schmidt, Ronald, Rodrick, G., 2003. Handbook Food Safety.
- Food handlers’ hygiene knowledge in small food businesses. Food Control. 2003;14(5):339-343.
- [CrossRef] [Google Scholar]
- WHO, 2017. No Title [WWW Document]. World Heal. Organ. WHO fact sheet. URL http://www.who.int/mediacentre/factsheets/fs399/en.
- Pre-requisites: A help or a hindrance to HACCP? Food Control. 2001;12:235-240.
- [CrossRef] [Google Scholar]
- Evidence Review on Regulation Culture and Behaviours”. Social Science Research Unit Report 37. London: Food Standards Agency; 2015.
- Intestinal parasites among food handlers of food service establishments in Ethiopia: a systematic review and meta-analysis. BMC Public Health. 2020;20(1):73.
- [CrossRef] [Google Scholar]
- Explaining the food safety behaviours of food handlers using theories of behaviour change: a systematic review. Int. J. Environ. Health Res.. 2018;28(3):323-340.
- [CrossRef] [Google Scholar]




