

Translate this page into:
Update on the genotyping distribution, epidemiology and associated risk factors in inflammatory disorder in adult subjects: A cross-sectional study
⁎Corresponding author at: Department of Zoology, College of Science, King Saud University, P.O. Box 2455, Riyadh, Saudi Arabia. shahidmahboob60@hotmail.com (Shahid Mahboob)
-
Received: ,
Accepted: ,
This article was originally published by Elsevier and was migrated to Scientific Scholar after the change of Publisher.
Peer review under responsibility of King Saud University.
Abstract
Limited molecular studies have been documented with ACE gene polymorphism in OA and RA in the major industrial city in the country. The current study aims to investigate the prevalence of the arthritis risks and perform the ACE gene polymorphism in OA and RA in hospital based population. In this hospital-based study, we adopted 1000 arthritis subjects; 539 was suffering with OA and 461 RA in the local hospital. Based on the filled questionnaire and signed consent form, patients were involved in this study. Genotyping was performed in 1000 arthritis subjects. Our results indicated the risk of BMI and smoking status in both OA and RA diseases. Most of the participants involved in this study were considered to opt the non-vegetarian rather than the vegetarian. The arthritis patients were interested in eating the chicken (65.7%) and then red meat (31.5%). Regular walking (22.4%) was found to be higher in the arthritis patients than the regular exercise (4.7%). However, males are more active than the females in both the regular exercise and regular walking. Most of the arthritis patients (37.3%) had the comfortable sleep duration between 9 and 10 h. The prevalence of arthritis has been increased and patients with high BMI should be growing the risks of the various arthritis. Simultaneously, weight gain is connected with both the OA and RA diseases. Physical activity is required to reduce the risks of arthritis. The present study recommends to avoid the smoking and maintain the normal BMI specifically in the females to avoid the arthritis disease in Faisalabad city in the Pakistan.
Keywords
Arthritis
Osteoarthritis
Rheumatoid arthritis
BMI
Regular exercise and physical activity

1 Introduction
Arthritis is defined as inflammation with chronic joint disorder affecting the joint(s) (Poornima et al., 2019). Rheumatic diseases denote approximately 200 conditions linked with joints, tendons, muscles, ligaments and bones (Mohsin et al., 2018). The process of inflammation is known to be the combination of leukocytes and immune proteins defend us from infections like virus and bacteria. Almost 100 enormous types of arthritis exist with appropriate sources and their specific treatments. Among arthritis; Rheumatoid and Osteo are well-known in humans. Both this arthritis varies in pathogeneses but displays phenotypic resemblances, overlapping cellular and molecular characteristics (Woetzel et al., 2014). Rheumatoid arthritis (RA) is known as progressive and autoimmune diseases allied with infections (Shi et al., 2019). It is also known as chronically inflammatory destructive joint disease with undocumented etiology (Okada, et al., 2019). The disease itself causes chronic synovial inflammation, ultimately leads to restricting joint destruction with systemic complications (Rodriguez-Carrio et al., 2019). The deficiency of RA disease is associated with worst outcomes (Hunter et al., 2017). The prevalence of RA varies between 0.15 and 0.61% (Hunter et al., 2017). Mainly, RA affects small joints in hands and feet, whereas, immune cells invade the lining of the joint, causing synovial inflammation and hyperplasia (Walsh et al., 2016). Since couple of decades, the progress in the treatment with RA is updating bizarrely (Tanaka, 2019). The second well-known arthritis is Osteoarthritis (OA), a progressive inflammatory low-grade disease entails in joint degradation. OA is also known as multifactorial disease, as one of the sub-types for arthritis. The disease is characterized by the progressive loss of articular cartilage in synovial joints which amends in adjacent bones. The disease OA mainly affects the knees, hands, hips and feet (Coimbra et al., 2019; Poornima et al., 2015). Among OA, Knee OA (KOA) is known to be a common chronic degenerative joint disease commonly affect the elder adults (Ganji, 2019). Bone cartilage is known to be important synergistic unit consisting area within deep layers of articular cartilage and underlying at subchondral bone (Poornima et al., 2018a). Bone shape in adults to be continued as affected by periosteal apposition, endosteal resorption, formation, resulting in substantial alteration of bone shape and size (Narloch and Glinkowski, 2019). Accurate etiology for the development of OA is still incomplete. However, the considered risks for OA are age, genetics, environmental factors and unhealthy lifestyle (Poornima et al., 2018b). Evidences for epidemiological studies indicates majorly obesity, aging, inflammation, genetic predisposition, and excessive mechanical load predisposes to development of OA (Subramanyam et al., 2016). In adults, the life-time risks with KOA is assumed to be 46% as per the Center for Disease control Kamal et al., 2017). Globally, prevalence of OA varies within the ethnicity due to the change in osteoarthritic along with age range between 40 and 70 years. Additionally, with obesity and overweight, the future threat may prone with other multifactorial diseases like cardiovascular diseases, type 2 diabetes, stroke and hypertension (Subramanyam et al., 2016). Both RA and OA are mostly the prevalent diseases in the joints. They are mainly occurred for pain and disability in a substantial proportion in the humans (Jahanban-Esfahlan et al., 2018). The prevalence of RA and OA are varying within the analogous populations. Globally, the prevalence of RA is 1% and in western population it is affected between 1 and 2%. In Pakistan, it shown between 0.5% (Akhter et al., 2011). The prevalence in Karachi is about 0.14% and 0.55% in Northern Karachi (Alam et al., 2011). There are limited studies have been carried out with RA and OA in different concepts of Pakistani population. But there are no epidemiological studies implemented from Faisalabad City in Pakistan. The present study aimed to investigate the hospital-based studies with a couple of arthritis and its similar affects with the onset of the disease in Pakistani Population.
2 Materials and methods
2.1 Questionnaire survey
The hospital based prospective study was carried out at Allied hospitals in Faisalabad, Pakistan during July 2014–January 2015. Ethical approval was obtained within the hospital locality. Randomly data was adopted by screening the arthritis patients by questionnaire. The data collected in the questionnaire consists of name, gender, age, type of arthritis, diagnosed age, allied disease, specific surgery and family histories along with and without consanguineous marriages. Another phase of the questionnaire consists of life-style details such as smoking, diet, physical activity and sleep duration. The third phase were documented with the risk factor specifics such as physical activity, exercises, injuries during exercises, infertility, overweight, obesity and natural aging diseases. The final phase of the questionnaire details was documented as education details along with socio-economic status. Based on the questionnaire survey and informed consent, we have selected 1000 participants among which 539 were osteoarthritis and 461 patients were rheumatoid arthritis.
2.2 Selection of Osteoarthritis patients
The osteoarthritis (OA) patients were recruited based on radio-graphical and clinical diagnosis in the department of orthopedics, allied hospital in Faisalabad district. For selection of OA patient, there is no blood test is involved, however, body mass index (BMI) will be selected as per Khan et al. (2019) equation. Unbearable joint pains were also one of the symptoms of OA. In this study, 254 males and 285 females of OA cases were selected of confirmed patients along with the signed consent form (Poornima et al., 2019).
2.3 Selection of Rheumatoid arthritis patients
In this study, 253 females and 208 males were selected the confirmed Rheumatoid arthritis (RA) cases in the hospital premises. The common symptoms of RA are swelling, pain and stiffness in joints. In these cases, also BMI was considered (Khan et al., 2019).
2.4 Statistical analysis
Mean and standard deviation was calculated with SPSS software (version 21.0).
3 Results
In this study 539 OA subjects; 52.9% (n = 285) were males and 47.1% (n = 254) female participants were involved and in RA, 461 individuals were recruited in which male participants were 54.9% (n = 253) and remaining 45.1% (n = 208) were female subjects (Fig. 1). The sex ratio/100 female of arthritic patients (100♀: 85.87♂). The sex ratio/100 females in OA was 100♀: 89.12♂ and in case of RA sex ratio/100 females was100♀: 82.21♂. The females were more affected (54.88%, 52.88%) than males (45.12%, 47.12%) in case of RA and OA patients, respectively (Fig. 1). The mean age of the OA patients was found to be 48.04 ± 0.43 and in RA it was 50.06 ± 0.44. The BMI in both the groups were found to be over-weight i.e., in OA was 25.96 ± 6.41 and in RA was 25.24 ± 6.28. The mean age of the diagnosis was found to be dissimilar in both OA (43.07 ± 0.39) and RA (44.84 ± 0.38). The maximum members were found to be high in the occupation in OA (68.3%; n = 368) when compared with RA (67.9%; n = 313). The smoking status was found to be high in OA (28.01%; n = 151) when compared with RA (25.6%; n = 118). The marital status was found to be low in RA (89.6%; n = 413) when compared with OA (92.2%; n = 497). The education status was found to be high in RA (54.9%; n = 253) when calculated with OA (46.8%; n = 252). The prevalence was other diseases was found to be 39% (n = 210) in OA and 28% (n = 129) in RA. All the participants were from Pakistani nativity. The complete details of the table were shown in Table 1.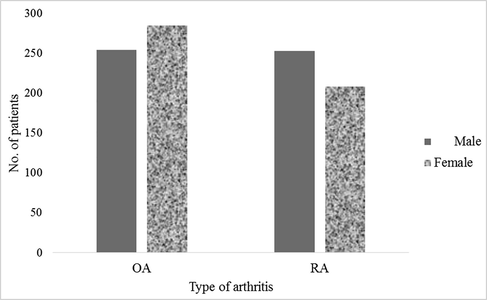
Percentage distribution of males and females among different types of arthritis.
Patient details
Osteoarthritis (n = 539)
Rheumatoid arthritis (n = 461)
Age
48.04 ± 0.43
50.06 ± 0.44
Gender (Male/Female)
52.9%/47.1%
54.9%/45.1%
Weight
64.4 ± 14.3
63.2 ± 14.9
Height
157.1 ± 10.6
158.4 ± 11.1
BMI
25.96 ± 6.41
25.24 ± 6.28
Mean age at diagnosis
43.07 ± 0.39
44.84 ± 0.38
Occupation
68.3%
67.9%
Smoking
28.01%
25.6%
Marital status
92.2%
89.6%
Education
46.8%
54.9%
Nationality
100%
100%
Other diseases
39%
28%
Family history
NA
NA
The details of the socio-economic status in arthritis patients been documented in the Table 2. The socio-economic status has been categorized into (i) lower class, (ii) middle class and (iii) upper class. The arthritis patients were majorly found to be middle class with 87.2%, followed by 9.6% in lower class and 3.2% in upper class. The similar type was found both in OA (M−91%, L-6.1% & U-2.8%) and RA (M−82.6%; L-13.7% & 3.7%) respectively.
Economic status
Arthritis (n = 1000)
Osteoarthritis (n = 539)
Rheumatoid arthritis (n = 461)
Lower class
96 (9.6%)
33 (6.1%)
63 (13.7%)
Middle class
872 (87.2%)
491 (91.1%)
381 (82.6%)
Upper class
32 (3.2%)
15 (2.8%)
17 (3.7%)
Total
1000 (100%)
539 (100%)
461 (100%)
In this study, we have recorded the details of dietary factor, which plays a major role in any human diseases. The status of diet was classified into vegetarian (V), non-vegetarian (NV) and mixed food (MF). The NV was reclassified into red-meat, chicken, fish and none has been confirmed as no details about specific meat in the Table 3. The V status in OA was found to be 9.8%, NV with 88.7% and MF with 1.5%; whereas in the RA more than 90% of the subjects were following the NV, then V for 8.7% and MF for 0.9%. In OA, the NV subjects were found to be high in opting chicken with 62.3%, 34.5% in red-meat; 1.8% in fish and 1.4% in none; however, in RA, 69.6% of the NV were interested in eating chicken, 28% in red meat,1.7% in fish and 0.7% in none.
Diet status
Osteoarthritis (n = 539)
Rheumatoid arthritis (n = 461)
Arthritis (n = 1000)
Vegetarian
53 (9.8%)
40 (8.7%)
93 (93%)
Non-vegetarian
478 (88.7%)
417 (90.4%)
895 (89.5%)
Mixed food
8 (1.5%)
4 (0.9%)
12 (12%)
Chicken
336 (62.3%)
321 (69.6%)
657 (65.7%)
Fish
10 (1.8%)
8 (1.7%)
18 (1.8%)
Red meat
186 (34.5%)
129 (28%)
315 (31.5%)
None
7 (1.4%)
3 (0.7%)
10 (1%)
Table 4 has been documented with physical activity and walking in both males and females in Arthritis subjects. Overall, 22.4% of the arthritis patients were found to be regular walking, whereas, 19.1% subjects were found to be irregular walking and 58.5% of the subjects were not involved in walking; among them males (25.5%) were more active than females (19.7%) in regular walking. In the irregular walking, females (16.2%) frequency was found to be low with the comparison of males (22.5%) and females with 64% were documented highly when compared with males (52%) for not involving in the walking. In arthritis patients, only 13% of the individuals were actively involved in regular (4.7%) and irregular (8.3%) in the physical activities; remaining 87% were not involved in the exercise. The 6.5% of male subjects were actively participated in the regular exercise; 9.5% in an irregular exercise and 84% of them were not involved in the exercises. The regular physical activity in the females were only 3.1%; irregular activity with 7.3% and 89.6% were found to be not elaborated in the exercises.
Activity
Arthritis patients (n = 1000)
Male subjects (n = 462)
Female subjects (n = 538)
Regular walking
224 (22.4%)
118 (25.5%)
106 (19.7%)
Irregular walking
191 (19.1%)
104 (22.5%)
87 (16.2%)
No walking
585 (58.5%)
240 (52%)
345 (64.1%)
Regular exercise
47 (4.7%)
30 (6.5%)
17 (3.1%)
Irregular exercise
83 (8.3%)
44 (9.5%)
39 (7.3%)
No exercise
870 (87%)
388 (84%)
482 (89.6%)
The duration of sleep in arthritis patients has been divided into; 5–6, 7–8, 9–10- & 11–12-hours duration. The 9–10 h of the sleep duration was found to be maximum in the arthritis patients for 37.3%; 33.1% of duration of sleep is for 7–8 h. The minimum of sleep duration for 5–6 h in arthritis patients was found to be 15.2% and 14.4% of the arthritis subjects will have the longest sleep for 11–12 h in a day. The maximum sleep duration in males (40.7%) and females (35.7%) were found to be between 9 and 10 and 7–8 h. The minimum of sleep duration was found commonly in both the genders between the 11–12 h of sleep, which was documented as a maximum sleep in the Table 5. The 14.7% and 30.1% of male subjects were found to be sleep duration between 5 and 6 and 7–8 h; whereas in the females, 5–6 h of the sleep duration has been documented with 15.6% and 35.7% for 7–8 h.
Sleep duration
Arthritis patients (n = 1000)
Male subjects (n = 462)
Female subjects (n = 538)
5–6 h
152 (15.2%)
68 (14.7%)
84 (15.6%)
7–8 h
331 (33.1%)
139 (30.1%)
192 (35.7%)
9–10 h
373 (37.3%)
188 (40.7%)
185 (34.3%)
11–12 h
144 (14.4%)
67 (14.5%)
77 (14.4%)
Genotypic distribution has been carried out with ACE ID gene polymorphism with OA and RA. Table 6 consists of allele and genotype frequencies. The genotype values in OA subjects were 22.3%-II, 39.3%-ID and 38.4%-DD and 41.9%-I and 58.1%-D alleles were documented. Under the other condition with RA, ACE genotypes were documented as follows; II-19.3%, ID-43.6% and DD-37.1% and allele frequencies were 41.1% in I and 58.9% in D-alleles respectively.
ACE gene
OA (n = 539)
RA (n = 461)
II genotypes
120 (22.3%)
89 (19.3%)
ID genotypes
212 (39.3%)
201 (43.6%)
DD genotypes
207 (38.4%)
171 (37.1%)
I allele
452 (41.9%)
379 (41.1%)
D allele
626 (58.1%)
543 (58.9%)
4 Discussion
The epidemiology of the present study was carried in Allied Hospitals in Faisalabad city in Pakistan. The current study was designed as the objective of patients were couple of arthritis diseases such as osteoarthritis and rheumatoid arthritis in the Pakistani population and genotyping was carried out with ACE genotypes. In this study, 1000 of total subjects were recruited which were classified as 539 subjects as OA and RA subjects were found to be 461 participants. Randomly OA subjects were found to be when compared with the RA. This indicates the prevalence of OA in Faisalabad city was proning presently. In our study, ID genotypes were found to be higher in both OA and RA which indicates as heterozygous genotypes may play a prominent role connected with the Arthritis diseases. Simultaneously, DD genotypes has found to be in maximum numbers. Our results indicate, genetics is connected with Arthritis in the Pakistani subjects.
Arthritis is a chronic joint disorder; known to be major and common cause of disability among adults. Globally, arthritis is documented as the fourth leading cause of physical disability (Fransen et al., 2011). Arthritis is termed as Inflammation, in general affects the joints in the human body. Numerous types of arthritis exist in the human body with variable causes and treatment methods. However, both RA and OA are found to be common in the global population (Mazur et al., 2019). The prevalence of arthritis in the Asian countries is found to be common with the highest prevalence rate in both Pakistan and India and varies in the characteristic differences in both the clinical features and laboratory analysis in the demonstration of the arthritis disease (Akhter et al., 2011). OA is known to be a degenerative disease occurs in the elder population. The disease may develop at any point of joint but majorly ripens in hip, face, knee and hand joints. Globally, the incidence of OA is high in women when compare with the men and the present study was found to be in accordance. The main risk factors of OAs are age, gender, socio-economic status, sedentary life-style, Genetics, obesity, nutritional factor, bone mass and smoking (Poornima et al., 2015). In Pakistan, OA is found to be common and it is due to high BMI and sedentary lifestyle (Iqbal et al., 2011; Liaqat et al., 2018; Sheikh et al., 2014). The prevalence of OA was found to high in females than the males in the world population and our studies were shown to be in accordance with the world population.
RA is known to be chronic systemic autoimmune disease arises mainly in females than the males; although commonly observed in elder population (Guo et al., 2018). However, there is a low prevalence of RA which is in the range between 0.5 and 1% in the general population with undocumented etiology, which is assumed with the combination of genetic and environmental factors (Karami et al., 2019). A vast difference was existed between the diagnosis and classification of RA in the patients. The diagnostic criteria do not exist for RA but mainly aimed for the therapeutic interventions and classification of RA do exists and the risks is lower when the classified criteria are used for clinical diagnosis (van der Woude and van der Helm-van Mil, 2018). Human leukocyte cells; neutrophils, mastocytes, T and B cells mainly contributes for the Pathogenesis of RA (Ren et al., 2019). There are limited studies have been carried out in the Pakistani population with RA and Mukhtar et al (Mukhtar et al., 2019) studies have been documented important predictor between the Vitamin D receptor and arthritis development.
There are limited genetic meta-analysis studies have been documented with both RA and OA diseases (Ebrahimiyan et al., 2019; Jackson et al., 2019). The present study has revealed the global significance association majorly with OA than the RA. In our study, all the participants were found to be in overweight. Although, BMI plays a major important role for the OA and RA diseases. Smoking, physical activities such as exercise and walking play an important role. Smoking is known to be one of the contradictory effects of risk factors for the arthritis (Felson and Zhang, 2015). However, Kong et al. (2017) meta-analysis studies also were in agreement with the combination of smoking in male OA patients. Chang et al. (2014) studies also confirm the smoking is a major risk factor for the RA male patients. However, in our study, the prevalence of smoking status was found to be high in OA (28%) than the RA (25.6%). Simultaneously, incidence of physical activities such as regular walking was documented in our study is to be 22.4% in the arthritis patients.
5 Conclusion
It has been concluded that the prevalence of arthritis has been increased and patients with high BMI should be growing the risks of the various arthritis. Simultaneously, weight gain is connected with both the OA and RA diseases. Physical activity is required to reduce the risks of arthritis. The present study recommends to avoid the smoking and maintain the normal BMI specifically in the females to avoid the arthritis disease in Faisalabad city in the Pakistan. Physical activities are required for the human body to maintain or reduce the risk of the diseases.
Acknowledgements
“The authors (KAAG, FAM and SM) express their sincere appreciation to the Researchers Supporting Project (RSP-2019-48), King Saud University, Riyadh, Saudi Arabia”.
Declaration of Competing Interest
The authors declare that they have no known competing financial interests or personal relationships that could have appeared to influence the work reported in this paper
References
- Prevalence of arthritis in India and Pakistan: a review. Rheumatol. Int.. 2011;31(7):849-855.
- [Google Scholar]
- Epidemiology of rheumatoid arthritis in a tertiary care unit, Karachi, Pakistan. J. Pak. Med. Assoc.. 2011;61(2):123-126.
- [Google Scholar]
- Smoking and rheumatoid arthritis. Int. J. Mol. Sci.. 2014;15(12):22279-22295. Epub 2014/12/06. doi: 10.3390/ijms151222279. PubMed PMID: 25479074; PubMed Central PMCID: PMCPMC4284707
- [Google Scholar]
- Generating evidence and understanding the treatment of osteoarthritis in Brazil: a study through Delphi methodology. Clinics (Sao Paulo, Brazil). 2019;74:e722
- [Google Scholar]
- Studying the association between STAT4 gene polymorphism and susceptibility to rheumatoid arthritis disease: an updated meta-analysis. Iranian J. Immunol.. 2019;16(1):71-83. Epub 2019/03/14. doi: 10.22034/iji.2019.39408. PubMed PMID: 30864557
- [Google Scholar]
- Smoking and osteoarthritis: a review of the evidence and its implications. Osteoarth. Carti.. 2015;23(3):331-333.
- [CrossRef] [Google Scholar]
- The epidemiology of osteoarthritis in Asia. Int. J. Rheum. Dis.. 2011;14(2):113-121.
- [CrossRef] [Google Scholar]
- Aromatherapy massage: a promising non-pharmacological adjuvant treatment for osteoarthritis knee pain. Korean J. Pain. 2019;32(2):133-134.
- [CrossRef] [Google Scholar]
- Rheumatoid arthritis: pathological mechanisms and modern pharmacologic therapies. Bone Res.. 2018;6:15. Epub 2018/05/08. doi: 10.1038/s41413-018-0016-9. PubMed PMID: 29736302; PubMed Central PMCID: PMCPMC5920070
- [Google Scholar]
- Prevalence of rheumatoid arthritis in the United States adult population in healthcare claims databases, 2004–2014. Rheum. Int.. 2017;37(9):1551-1557.
- [CrossRef] [Google Scholar]
- Frequency of factors associated with knee osteoarthritis. J. Pak. Med. Assoc.. 2011;61(8):786-789.
- [Google Scholar]
- Arthritis self-efficacy beliefs and functioning among osteoarthritis and rheumatoid arthritis patients: a meta-analytic review. Rheumatology (Oxford, England) 2019 Epub 2019/06/19. doi: 10.1093/rheumatology/kez219. PubMed PMID: 31211379
- [Google Scholar]
- Melatonin in regulation of inflammatory pathways in rheumatoid arthritis and osteoarthritis: involvement of circadian clock genes. British J. Pharmacol.. 2018;175(16):3230-3238.
- [CrossRef] [Google Scholar]
- Radiological and biochemical effects (CTX-II, MMP-3, 8, and 13) of low-level laser therapy (LLLT) in chronic osteoarthritis in Al-Kharj, Saudi Arabia. Lasers Med. Sci.. 2017;32(2):297-303.
- [Google Scholar]
- Genetic implications in the pathogenesis of rheumatoid arthritis; an updated review. Gene. 2019;702:8-16.
- [CrossRef] [Google Scholar]
- Genetic confirmation of T2DM meta-analysis variants studied in gestational diabetes mellitus in an Indian population. Diabetes Metabol. Synd.. 2019;1:688-694.
- [Google Scholar]
- Association between smoking and risk of knee osteoarthritis: a systematic review and meta-analysis. Osteoarth. Carti.. 2017;25(6):809-816. Epub 2016/12/25. doi: 10.1016/j.joca.2016.12.020. PubMed PMID: 28011100
- [Google Scholar]
- Prevalence of knee osteoarthritis and quality of life in middle aged adults. IJRS. 2018;7(02):26-28.
- [Google Scholar]
- Interpersonal correlates of the tendency to seek help in the situation of indebtedness in healthy people and in patients with impaired mobility, related to chronic disorders of the locomotor system–Pilot study. Annals Agri. Env. Med. 2019
- [CrossRef] [Google Scholar]
- Prevalence of rheumatic diseases in a tertiary care hospital of Karachi. Cureus. 2018;10(6):e2858
- [CrossRef] [Google Scholar]
- Vitamin D receptor gene polymorphism: an important predictor of arthritis development. Biomed. Res. Int.. 2019;18(2019):8326246. eCollection
- [CrossRef] [Google Scholar]
- Osteoarthritis changes hip geometry and biomechanics regardless of bone mineral density-a quantitative computed tomography. Study. J. Clin. Med.. 2019;8(5)
- [CrossRef] [Google Scholar]
- Genetics of rheumatoid arthritis: 2018 status. Annals Rheum. Dis.. 2019;78(4):446-453. Epub 2018/12/12. doi: 10.1136/annrheumdis-2018-213678. PubMed PMID: 30530827
- [Google Scholar]
- The insertion and deletion (I28005D) polymorphism of the angiotensin I converting enzyme gene is a risk factor for osteoarthritis in an Asian Indian population. J. Renin-Angiotensin-Aldosterone Sys:. JRAAS. 2015;16(4):1281-1287.
- [Google Scholar]
- Poornima, S., Subramanyam, K., Iyer, G., Darooei, M., Daram, S., Sumanlatha, G.J.A.O, 2018a. Association of TGFβ1 gene polymorphisms with early onset primary knee osteoarthritis in South Indians: case-control study from a cosmopolitan city. 3 (1), 1007.
- Genetic association of GDF5, COG5 and CYBA gene polymorphisms with primary knee osteoarthritis in South Indian population. Gen. Mol. Biol. Res.. 2018;1(1 5)
- [Google Scholar]
- Role of SREBP2 gene polymorphism on knee osteoarthritis in the South Indian Hyderabad Population: a hospital based study with G595C variant. J. Ortho.. 2019;16(3):293-297.
- [Google Scholar]
- Association between interleukin-21 gene rs6822844 polymorphism and rheumatoid arthritis susceptibility. Biosci. Rep.. 2019;39(8) Epub 2019/08/02. doi: 10.1042/bsr20190110. PubMed PMID: 31366568; PubMed Central PMCID: PMCPMC6695501
- [Google Scholar]
- Vitamin D receptor polymorphism and DHCR7 contribute to the abnormal interplay between Vitamin D and lipid profile in rheumatoid arthritis. Sci. Rep.. 2019;9(1):2546.
- [CrossRef] [Google Scholar]
- Postural risk factors for Osteoarthritis in Pakistani Women. Int. Inv. J. Med. Medi. Sci.. 2014;1(4):46-49.
- [Google Scholar]
- Infection risks of rituximab versus non-rituximab treatment for rheumatoid arthritis: a systematic review and meta-analysis. Int. J. Rheum. Dis.. 2019;22(8):1361-1370.
- [CrossRef] [Google Scholar]
- Subramanyam, K., Poornima, S., Juturu, K.K., Anand, D., Mohanthy, S., Hasan, Q.J.G.R., 2016. Missense FokI variant in the vitamin D receptor gene in primary knee osteoarthritis patients in south Indian population. 4, 118–122.
- Tanaka, S., 2019. RankL is a therapeutic target of bone destruction in rheumatoid arthritis. F1000Research. 8. Epub 2019/05/10. doi: 10.12688/f1000research.17296.1. PubMed PMID: 31069051; PubMed Central PMCID: PMCPMC6480939.
- Update on the epidemiology, risk factors, and disease outcomes of rheumatoid arthritis. Best Prac. Res. Clin. Rheumatol.. 2018;32(2):174-187. Epub 2018/12/12. doi: 10.1016/j.berh.2018.10.005. PubMed PMID: 30527425
- [Google Scholar]
- Integrative genomic deconvolution of rheumatoid arthritis GWAS loci into gene and cell type associations. Genome Biol.. 2016;17:79. Epub 2016/05/04. doi: 10.1186/s13059-016-0948-6
- [Google Scholar]
- Identification of rheumatoid arthritis and osteoarthritis patients by transcriptome-based rule set generation. Arthritis Res. Ther.. 2014;1 16(2):R84.
- [CrossRef] [Google Scholar]




