

Translate this page into:
Understanding and treating suboptimal health status through tourism engagement: An exploratory study of Chinese domestic tourists
⁎Corresponding author. zdn@fudan.edu.cn (Danni Zheng),
-
Received: ,
Accepted: ,
This article was originally published by Elsevier and was migrated to Scientific Scholar after the change of Publisher.
Abstract
Objectives
Suboptimal health status (SHS) is a global public health concern of worldwide academic interest. The topic is popular in the medical sciences, including public health; however, other disciplines have paid little attention to this condition despite aging societies. This study introduced SHS into the tourism literature, a logical connection given the established positive correlation between well-being and tourism engagement. Lifestyle factors are crucial to SHS. Accordingly, this study examines tourists’ sociodemographic characteristics, tourism-related attributes, and lifestyle behaviors to compare individuals with SHS to those with optimal health status.
Methods
Chinese tourists in Shandong Province, China who had visited Mount Tai within 6 months of study recruitment (October to December 2021) completed a pen-and-pencil survey to answer questions for this cross-sectional research study. In total, 360 surveys were eligible for analysis following initial screening.
Results
The self-report SHS status survey, SHSQ-25, was used to determine the portion of study participants exhibiting symptoms of SHS. The descriptive analysis indicated that 36.4 % (n = 131) of the sample (N = 360) presented with SHS. Three lifestyle behavior factors (i.e., work stress, sleep length, and drinking length), five SHS domains (i.e., fatigue, cardiovascular system, immune system, digestive system, and mental status), and two tourism-related attributes (i.e., international travel frequency and travel expenditure) were integrated using canonical correlation analysis to determine relationships among these three domains.
Conclusions
Results from this study demonstrated the meaningful relationships among lifestyle behaviors, tourism-related attributes, and SHS. Previous work has implied that tourism participation may enhance individuals’ health status and well-being; however, conclusions from this study are contradictory to those findings. For travelers with SHS to fully benefit from tourism, more information is needed to develop suitable marketing strategies and tourism products. This study provides a starting point to direct future research to further explore motivations of and strategies to benefit tourists with SHS.
Keywords
Suboptimal health status
Lifestyle behaviors
Optimal health
Tourist health
Interdisciplinary
China

1 Introduction
Health reflects a living organism’s functional or metabolic efficiency. In humans, health is the overall condition of one’s mind and body; healthy people are often free of illness, stress, injury, or pain (Wang and Yan, 2012). Per the World Health Organization (WHO) (1946), health is “a state of complete physical, mental, and social well-being and not merely the absence of disease or infirmity.” The prevalence of stress in modern society has led to reports of poor health without an explicit diagnosis, a state otherwise termed “suboptimal health status” (SHS) (Yan et al., 2009, 2012). SHS embodies a middle ground between health and disease (Yan et al., 2009), characterized by ambiguous health complaints, general weakness, and a lack of vitality. SHS is also thought to contribute to chronic illness; examples include anxiety or depression, headache, chronic fatigue, and digestive issues (Hou et al., 2018; Wang, 2020; Wang and Tan, 2019; Wang et al., 2016; Wang et al., 2017, 2021; Yan et al., 2012; Yan et al., 2015).
Traditional Chinese medicine has long focused on the physical attributes distinguishing health and disease, birthing the notion of SHS (Liang et al., 2018). SHS is a global health problem of practical and academic concern (e.g., Adua et al., 2019). As an example, China’s economic and social landscape has shifted drastically over the past several decades. These changes have heightened the incidence of major chronic diseases (Wang et al., 2005). Economic development has led residents to be stressed at home, school, and work, further elevating the risk of SHS (Wang et al., 2021). Statistics suggest that 55 %–75 % of Chinese adults have SHS (e.g., Ma et al., 2018; Xu et al., 2020). In 2014, SHS was reported to apply to 46.0 % of respondents surveyed in southern China (Chen et al., 2014). Some risk factors related to SHS (including unbalanced diets, minimal exercise, and drug/alcohol use) have been intensified because of urbanization (Wang et al., 2021). Although researchers in the life sciences continue to explore SHS, no study has pertained to lifestyle differences between people with SHS and optimal health status (OHS) in the Chinese population to address individual well-being.
Tourism scholars have started to ponder the link between tourism and well-being with regard to health promotion (Coghlan, 2015; Smith and Diekmann, 2017). Research contexts have included rural well-being tourism (Pesonen and Komppula, 2010), team tourism (Su and Zhang, 2020), and family adventure tourism (Pomfret, 2021). There is an increased interest in learning more about the possible ties between tourism and people’s health status, partially driven by so many modern-day health concerns, including aging (Qiao et al., 2022). Most work to this point has concentrated on tourists with assumingly good health; however, a few notable exceptions exist. Levi et al. (2019) studied tourists with symptoms of depression. More recently, Wen et al. (2022) argued that no tourism or medical research has explored travel in relation to dementia treatment. They critically reviewed the tourism and dementia literature, concluding that tourism should be considered as a potential dementia intervention to enhance patients’ well-being. Studies have not yet explored specific tourism-related behaviors of people with SHS.
Tourism is vulnerable to occurrences such as disease outbreaks, natural disasters, and political events (Zheng et al., 2021, 2022). For example, COVID-19 has pervaded the tourism sector around the world, including China, and it has in turn influenced Chinese tourists’ consumption (Wen et al., 2021b). The pandemic has also exacerbated mental health concerns, calling for more careful investigation of personal wellbeing. When considering emerging tourist groups, such as those with health concerns, sociodemographics (e.g., trip purpose, travel preferences, travel frequency, and trip length) can provide useful behavioral information. These variables have been adopted to predict tourists’ shopping decisions (Oh et al., 2004), perceived destination personality and visitors’ emotional experiences (Šagovnovic and Kovacic, 2021), perceived destination image (Beerli and Martin, 2004), and ecofriendly attitudes (Leonidou et al., 2015). To date, there has been very little research exploring relationships between tourism and SHS (versus OHS) in terms of specific groups’ sociodemographic and tourism-related attributes. This research used a Chinese sample to quantify these potential relationships. Lifestyle factors are closely tied to SHS (Xue et al., 2021), so this study included questions about sociodemographic characteristics, tourism-related attributes, and lifestyle behaviors in the survey instrument so travelers with SHS could be compared to those with OHS. Results shed light on respective tourism participation and associations with health status. These findings contribute to the development of strategies tailored to an emerging but neglected tourist segment (i.e., tourists with SHS). Implications can additionally inspire public health scholars to enhance individuals’ health status and well-being through tourism engagement. Moreover, this research provides methodological contributions by canonical correlation analysis (CCA) based on quantitative data related to the following objectives:
-
to compare tourism-related characteristics and lifestyle behaviors (i.e., work stress level, daily physical activities, frequency and length of smoking and drinking, and diet) of tourists with SHS and OHS;
-
to identify relationships between SHS and lifestyle behaviors and tourism-related characteristics, respectively; and
-
to identify relationships among lifestyle behaviors, tourism-related characteristics, and SHS.
2 Methodology
2.1 Research design and respondents
A cross-sectional study was launched and data was collected between October and December 2021 in Shandong Province, China to achieve the proposed objectives. Local Chinese tourists who had visited Mount Tai within the past 6 months completed the survey on site. Mount Tai is a World Cultural Heritage Site with heavy visitation (Zhu et al., 2022). Data screening was performed by checking for outliers, errors, and missing data. As a result, 360 surveys were retained for formal analysis. Skewness values ranged from −0.129 to 0.846. Kurtosis values were between 1.688 and 0.462. Normality was therefore not an issue in this research (Kline, 2015).
2.2 Measurements
Surveys were modeled after other studies on tourism and suboptimal health to collect data on respondents’ personal attributes and demographics. The questionnaire consisted of three main sections (numbers 2 through 4 below) following the collection of basic demographic information:
-
Sociodemographic information, including respondents’ gender, age, education, employment, and income level.
-
Lifestyle behavior factors, including work stress (5-point scale: 1 = very mild; 5 = very severe), daily physical activity (4-point scale: 1 none; 4 = intense), sleep length (i.e., number of hours slept per day), smoking behavior (frequency and length of smoking), drinking behavior (frequency and length of drinking), and dietary habits (5-point scale: 1 = vegetarian; 5 = meatatarian). All of these factors were drawn from Xue et al. (2021) and Yan et al. (2009).
-
Tourist characteristics, including domestic and international travel frequency (8-point scale: 1 = none; 8 = over 6 times), travel types (e.g., sightseeing, shopping, leisure and entertainment, business), and extent of travel (6-point scale: 1 = very mild; 6 = very intense); transportation modes (airlines, train, self-driving, bus, other); and domestic and international travel length (4-point scale: 1 = 1–2 days; 4 = over 14 days), preference (alone, with family, with friends, with unfamiliar tourists, other), and expenditure (6-point scale: 1 = below 1000 yuan; 6 = above 20,000 yuan).
-
The self-report suboptimal health status survey SHSQ-25 (Yan et al., 2009) was used to assess respondents’ sociodemographics and SHS. The SHSQ-25 covers five dimensions measuring individuals’ fatigue (9 items), cardiovascular system (3 items), digestive system (3 items), immune system (3 items), and mental status (7 items). Respondents were asked to score each statement on a 5-point Likert-type scale (1 = never or almost never; 5 = always). The scores of 1 to 5 were re-coded as 0 to 4 (Wang and Yan, 2012). Based on the SHSQ-25 criterion (Yan et al., 2012), respondents’ health status was categorized into two groups: an SHS group (total score ≥ 35) and an optimal health group (OPH; total score < 35).
2.3 Data analyses
Data were analyzed in SPSS (IBM, V23, Chicago). Mean scores and frequencies were computed to summarize the descriptive statistics. Independent-sample t-tests were conducted to identify potential statistical differences between SHS and OPH groups based on lifestyle behaviors and tourism-related characteristics. CCA (SPSS23 syntax commands) was carried out to explore relationships between latent variables in the variable sets regarding respondents’ lifestyle behaviors, tourist characteristics, and SHS. As CCA can combine observed dependent and independent variables into a single synthetic (or latent) construct, it provides a maximum simple correlation for two sets of variables (Hair, 2010).
3 Results
3.1 Participants
Respondents’ sociodemographic characteristics are listed in Table 1. Overall, 131 (36.4 %) respondents were recognized as having SHS, whereas 229 (63.6 %) had OPH. A large proportion of young women aged between 18 and 24 were categorized as having SHS. By contrast, the OPH prevalence was high among young men between 25 and 34 years old. Most of OPH respondents (70.7 %) and SHS respondents (73.3 %) had a college or university education. Many SHS respondents (54.2 %) earned below 5,000 yuan per month, while the proportion was higher in the OPH group (60.3 %). However, the SHS group featured a greater proportion of married and high-income respondents (i.e., those earning more than 8,001 yuan/month) compared with the OPH group. These proportions accounted for 34.4 % and 32.3 % (married) and 19.1 % and 16.2 % (high-income) of the respective groups. Note. OPH = optimal health status; SHS = suboptimal health status.
Characteristics
Frequency
Percentage
SHS
OPH
Total
SHS
OPH
Total
Gender
Male
43
126
169
38.8
55.0
46.9
Female
88
103
191
67.2
44.9
53.1
Age
18–24
67
96
163
51.1
41.9
45.3
25–34
47
99
146
35.9
43.2
40.6
35–49
16
24
48
12.2
14.0
13.3
50 or above
1
2
3
0.8
0.9
0.8
Marital Status
Unmarried
86
155
241
65.6
67.7
66.9
Married
45
74
119
34.4
32.3
33.1
Education
Junior primary/High school
28
58
15
21.4
25.3
4.2
College/University
96
162
106
73.3
70.7
29.4
Master or above
7
9
16
5.3
3.9
4.4
Employment
Full-time
82
140
222
62.6
61.1
61.7
Part-time
10
18
28
7.6
7.9
7.8
Self-employed
20
32
52
15.3
14.0
14.4
Unemployed
19
39
58
14.5
17.0
16.1
Income Level
Below ¥5000
71
138
209
54.2
60.3
58.1
¥5001–8000
35
54
89
26.7
23.6
24.7
¥8001 or above
25
37
62
19.1
16.2
17.2
Total
131
229
360
36.4
63.6
100
3.2 Comparison between SHS and OPH groups
No statistically significant differences were observed in smoking behavior, drinking frequency, dietary habits, and most tourist characteristics between the SHS and OPH groups; however, mean scores on work stress (3.53 vs 3.19, t = 4.26, df = 398, p < 0.001), drinking length (3.73 vs 2.35, t = 2.89, df = 398, p = 0.004), international travel frequency (1.26 vs 1.09, t = 2.17, df = 398, p = 0.003), and travel expenditure (2.43 vs 2.11, t = 3.00, df = 398, p = 0.003) were significantly higher in the SHS group than in the OPH group. Conversely, respondents with SHS reported less daily physical activity (1.92 vs 2.19, t = -3.12, df = 398, p = 0.016) and shorter sleep duration (7.19 vs 7.47, t = -2.44, df = 398, p = 0.016) than OPH respondents. Specifically, 60 % of SHS respondents slept<8 h per day versus 49 % in the OPH group (Figs. 1 and 2). Sightseeing accounted for the most common travel type among respondents with OPH (44.6 %); leisure and entertainment purposes were most frequent in the SHS group (29 %). Regarding travel preferences, more SHS respondents preferred to travel alone (10.7 % vs 8.1 % for domestic travel; 7.0 % vs 5.9 % for international travel), whereas more OPH respondents chose to travel with family (40.7 % vs 41.9 % for domestic travel; 42.5 % vs 46.2 % for international travel) (Figs. 3 and 4).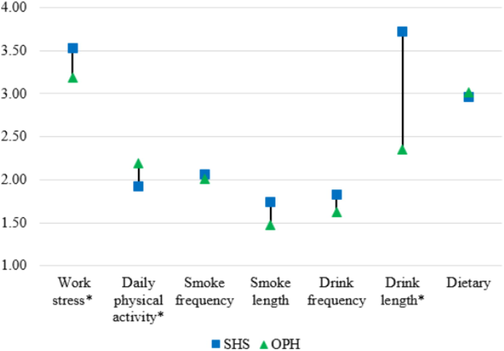
Mean score comparison between SHS and OPH groups in lifestyle behaviors. Note. * = significant difference in independent-sample t-tests.
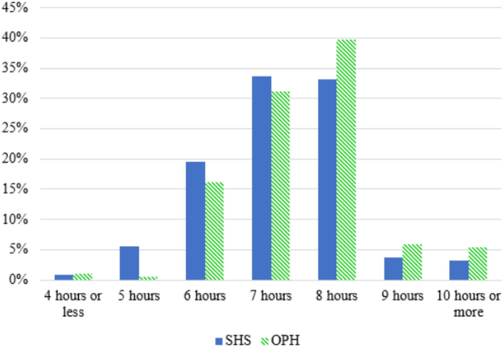
Comparison between SHS and OPH groups in daily sleep length.
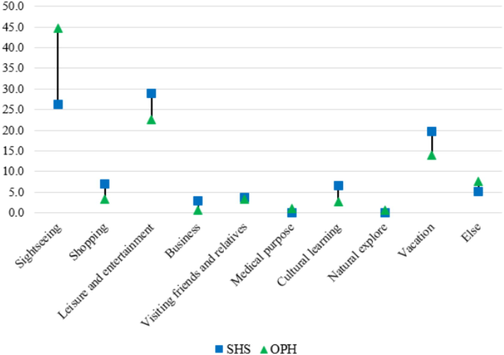
Comparison between SHS and OPH groups in travel types. Note: “Else” represents other travel types that were not listed in the survey.
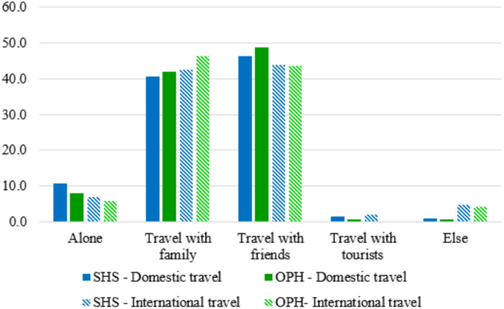
Comparison between SHS and OPH groups in domestic and international travel preferences. Note: “Else” represents other travel preferences that were not listed in the survey.
3.3 Relationships between lifestyle behaviors and suboptimal health status
The full CCA model demonstrated associations between predictor variables (i.e., life states) and criterion variables (i.e., fatigue, cardiovascular system, digestive system, immune system, and mental status). Five functions were generated in the CCA model [Wilks’ λ = 0.723, F (3,1689) = 40.00, p < 0.001], indicating significant relationships between lifestyle behaviors and these five SHS dimensions. The r2 type effect size was 0.277, explaining 27.7 % of the variance in the full model. Only the first two functions were statistically significant. According to the Rc2 effect (squared canonical correlations) cut-off value (Tabachnick and Fidell, 2014), Root 2 [Wilks’ λ = 0.884, F(2, 1400) = 28.00, p < 0.01] was deleted as its Rc2 value was below 0.1.
Canonical loadings indicated the correlations between each variate and canonical variable. Significant variables in the two sets were identified based on the recommended threshold of 0.4 (Sherry and Henson, 2005). The most significant predictor variables included work stress, sleep duration, and drinking length. All five SHS dimensions (i.e., fatigue, cardiovascular system, digestive system, immune system, and mental status) were salient criterion variables. In particular, SHS was positively related to work stress (rs = -0.74) and drinking length (rs = -0.43) but negatively related to sleep duration (rs = 0.49) (Table 2 and Fig. 5). Note. rs = structure coefficients (canonical loadings); rs2 = squared structure coefficients; h2 = communality coefficient. rs values greater than 0.40 are in bold; ***p < 0.001.
Variables
Function 1
rs
rs2 (%)
h2 (%)
Predictor variables – Life state
Work stress
−0.74
54.17
54.76
Daily physical activity
0.36
13.18
12.96
Sleep length
0.49
23.91
24.01
Smoking frequency
0.04
0.14
0.16
Smoking length
−0.09
0.88
0.81
Drinking frequency
−0.22
5.02
4.84
Drinking length
−0.43
18.58
18.49
Diet
−0.25
6.40
6.25
Criterion variables – Suboptimal health status
Fatigue
−0.94
88.17
88.36
Cardiovascular system
−0.60
35.76
36
Digestive system
−0.76
57.30
57.76
Immune system
−0.60
35.64
36
Mental status
−0.85
72.42
72.25
Canonical correlation
0.427***
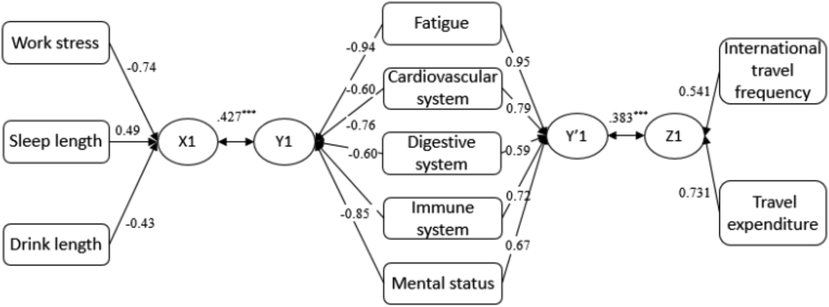
Canonical correlations between lifestyle behaviors, tourist characteristics, and suboptimal health status. Note. X1 = lifestyle behavior canonical variables; Y1, Y’1 = SHS canonical variables; Z1 = tourist characteristic canonical variables. Only variables with canonical loadings > 0.4 are presented.
3.4 Relationships between tourist characteristics and suboptimal health status
CCA was further performed to reveal potential relationships between tourist characteristics and SHS. Results generated one meaningful function [Wilks’ λ = 0.756, F (2,1759) = 50.00, p < 0.001], contributing to 24.4 % of the variance between the two sets of variables. The canonical correlation of Root 1 was 0.383, reflecting a slight correlation between the combination of tourist characteristics and the linear combination of SHS variables (p < 0.001). Canonical loadings of the five SHS dimensions were above the 0.4 cut-off; among tourist characteristics, only international travel frequency and travel expenditure met this criterion. Results also showed that international travel frequency (rs = 0.54) and travel expenditure (rs = 0.73) were positively related to respondents’ fatigue (rs = 0.95), cardiovascular system (rs = 0.79), digestive system (rs = 0.59), immune system (rs = 0.72), and mental status (rs = 0.67) (Table 3 and Fig. 5). Note. rs = structure coefficients (canonical loadings); rs2 = squared structure coefficients; h2 = communality coefficient. rs values greater than 0.40 are in bold; ***p < 0.001.
Variables
Function 1
rs
rs2 (%)
h2 (%)
Predictor variables – Tourist characteristics
Domestic travel frequency
0.10
0.96
0.96
International travel frequency
0.54
29.27
29.27
Travel type
0.13
1.56
1.56
Travel extent
0.27
7.40
7.40
Travel transportation
0.17
2.82
2.82
Domestic travel length
0.04
0.18
0.18
Intentional travel length
0.07
0.46
0.46
Domestic travel preference
−0.12
1.46
1.46
International travel preference
0.19
3.50
3.50
Travel expenditure
0.73
53.44
53.44
Criterion variables – Suboptimal health status
Fatigue
0.95
89.68
89.68
Cardiovascular system
0.79
61.62
61.62
Digestive system
0.59
34.57
34.57
Immune system
0.72
51.12
51.12
Mental status
0.67
44.76
44.76
Canonical correlation
0.383***
4 Discussion
Previous research on the topic of SHS related to tourism and public health is scarce, and this is one of the first studies to explore this concept. This cross-sectional study used a sample of Chinese domestic tourists to identify 1) differences between tourists with SHS and OHS based on lifestyle behaviors and sociodemographics; 2) associations between lifestyle behaviors and sociodemographics among tourists with SHS; and 3) relationships among lifestyle behaviors, sociodemographics, and SHS. Findings help to clarify the important but neglected concept of SHS in social science. Specific insights are detailed below.
First, the descriptive analysis unexpectedly indicated that 36.4 % (n = 131) of the tourist sample (N = 360) exhibited symptoms of SHS based on their responses to the SHSQ-25 (Yan et al., 2009). Xue et al. (2021) already established the serious nature of SHS in society by reporting a prevalence of SHS exceeding 65 % in China. As displayed in Table 1, the number of female respondents with SHS (n = 88) exceeded that of men (n = 43) by 104.65 %; that is, women appear to suffer from SHS more than men. This pattern accords with Bi et al.’s (2014) discovery that female students in China displayed a poorer health status than their male counterparts. The current study thus provides empirical evidence showing that female tourists’ SHS is especially concerning. From a practical standpoint, this data could motivate tourism marketing staff to highlight the importance of health in their marketing strategies. This may even lead to products and programs that are specifically intended to enhance the health and well-being of people with SHS.
In addition, our work presents a preliminary comparison of tourists with SHS and OHS based on certain lifestyle behaviors and sociodemographic variables using a Chinese sample. Intense work stress and a longer drinking length were found to significantly contribute to SHS, consistent with previous research (e.g., Xue et al., 2021; Yan et al., 2009, 2012). Interestingly, more frequent international travel and higher travel expenditure were positively associated with SHS as well. The COVID-19 pandemic could partly explain this trend given the virus’s effects on individuals’ stress levels (Mondo et al., 2021), fear of infection (Ahorsu et al., 2020), perceived risk (Yıldırım and Güler, 2022), and avoidance of international travel (Chua et al., 2021). These circumstances could jointly affect tourists’ mental and physical health. Unique medical considerations further apply to specific tourist segments’ international travel (Freedman et al., 2016), such as senior tourists and tourists with psychological disorders (Levi et al., 2019; Wen et al., 2022; Zhao et al., 2021). In terms of the association between higher travel expenditure and SHS, individuals who can normally afford to travel internationally might hold decent jobs and earn a fair salary in China – but they are also likely to face persistent pressure from work and family that can contribute to SHS. Conversely, tourists with OHS in this study tended to have good lifestyle habits (e.g., more daily physical activity and longer sleep), consistent with Xue et al. (2021). Tourists with OHS generally preferred sightseeing and being close to nature. Those with SHS favored leisure and entertainment, presumably for stress relief.
Moreover, as illustrated in Fig. 5, the CCA results integrating lifestyle behavior factors (i.e., work stress, sleep length, and drinking length), five domains of SHS (i.e., fatigue, cardiovascular system, digestive system, immune system, and mental status), and two tourism-related attributes (i.e., international travel frequency and travel expenditure) paint a full picture of relationships among these three constructs. Chinese tourists across all SHS domains benefited from a healthy lifestyle (i.e., low work-related stress, adequate sleep, and limited substance use). Work stress is a known risk factor for cardiovascular disease (Kivimäki and Kawachi, 2015) and mental health issues (Humpel and Caputi, 2001). High-quality sleep is essential to physical health, with sleep disorders generally being detrimental (Wells and Vaughn, 2012); for instance, sleep deprivation can contribute to infertility (Lateef and Akintubosun, 2020). Frequent binge drinking is associated with poor mental health in terms of depression, emotional instability, and stress, all of which detract from one’s quality of life (McDevitt-Murphy et al., 2010; Okoro et al., 2004). International travel frequency and travel expenditure were shown to adversely influence tourists’ SHS, contradicting previous studies that framed tourism as a way to improve people’s mental and physical health (Levi et al., 2019; Wen et al., 2022). These findings also counter studies demonstrating that tourism experiences foster mindfulness and happiness (Gao and Kerstetter, 2018). Treatments based in positive psychology show promise in enhancing the well-being of people with SHS, but more work is needed to discern how to incorporate these strategies into tourism experiences.
5 Conclusion
Suboptimal health status is a public health concern that has not been widely considered in previous tourism-related studies. This cross-sectional study of Chinese domestic travelers explored the relationships among lifestyle behaviors, tourism-related attributes, and SHS. Not surprisingly, positive lifestyle behaviors were assiciated with low scores in the five SHS domains (therefore, positive lifestyle behaviors indicated better health status). In addition, two tourism-related attributes were also positvely associated with these domains, providing insight for tourism and public health practitioners. Given the seemingly contradictory finding in this study showing that tourism participation may not benefit individuals’ health status and overall well-being, more work is needed to develop and implement marketing strategies and tourism products to help travelers with SHS get the most out of tourism experiences. This study serves as a starting point for future scholars to design additional studies to gain more knowledge about tourists with SHS. It would be interesting for medical scientists to get involved to compare tourists with SHS to those with OHS in clinical studies. Scholars specializing in the social sciences could conduct interview-style qualitative studies in conjunction with medical scientists to gather data about trip preferences for tourists with SHS. Interdisciplinary approaches (e.g., between marketing, medical science, and tourism) can bridge the medical and social sciences to address societal issues such as SHS (Wen et al., 2022). Personal health has become a popular topic amid global crises such as COVID-19 and ongoing wars. Interdisciplinary efforts in this vein can offer implications to promote well-being (Wen et al., 2021a; Wen et al., 2021c). Cultural values are also important to consider when examining the travel behavior of people with SHS. This concept was drawn from traditional Chinese medicine but has recently been applied to broader populations. As research continues, including cultural factors may generate more inclusive models. Lastly, in today’s aging society, tourism could help to alleviate related issues (e.g., psychological disorders such as depression and dementia). Relevant studies can inform tourism practioners about positioning their products to enhance well-being (Wen et al., 2022). Last, our use of an exclusively Chinese sample limits findings’ generalisability. Future research should include diverse participants to shed further light on the nexus between tourism engagement and SHS.
Author contribution statement
Dr. Jun Wen: conception and design; data collection; draft the manuscript; critically revise the manuscript; and give final submission approval.
Dr. Danni Zheng: conception and design; data analysis; draft the manuscript; critically revise the manuscript; and give final submission approval.
Prof. Ian Phau: critically revise the manuscript; and final submission approval.
Sources of funding
This work was supported by Dr. Jun Wen’s High-Achieving Researcher Scheme Funding 2021 from Edith Cowan University; This work was supported by Dr. Danni Zheng’s the National Natural Science Foundation of China [Grant No 72102045].
Ethical approval statement
This study was approved by the Ethics Committee of Edith Cowan University (2021-03138-WEN).
Data availability statement
The data are available from the corresponding authors on the reasonable request.
Authors’ statement
Author confirm that no subsequent addition of authors' names will be permitted by the journal.
Declaration of Competing Interest
The authors declare that they have no known competing financial interests or personal relationships that could have appeared to influence the work reported in this paper.
References
- Utilization of N-glycosylation profiles as risk stratification biomarkers for suboptimal health status and metabolic syndrome in a Ghanaian population. Biomarkers Med.. 2019;13(15):1273-1287.
- [Google Scholar]
- The fear of COVID-19 scale: Development and initial validation. Int. J. Mental Health Addict. 2020
- [CrossRef] [Google Scholar]
- Tourists’ characteristics and the perceived image of tourist destinations: a quantitative analysis—a case study of Lanzarote, Spain. Tour. Manage.. 2004;25(5):623-636.
- [Google Scholar]
- Association of lifestyle factors and suboptimal health status: a cross- sectional study of Chinese students. BMJ Open. 2014;4(6):e005156.
- [Google Scholar]
- Associations between breakfast eating habits and health-promoting lifestyle, suboptimal health status in Southern China: A population based, cross-sectional study. J. Transl. Med.. 2014;12(1)
- [Google Scholar]
- Impact of health risk perception on avoidance of international travel in the wake of a pandemic. Curr. Issues Tour.. 2021;24(7):985-1002.
- [Google Scholar]
- Tourism and health: using positive psychology principles to maximise participants’ wellbeing outcomes – a design concept for charity challenge tourism. J. Sustain. Tour.. 2015;23(3):382-400.
- [Google Scholar]
- Medical considerations before international travel. N. Engl. J. Med.. 2016;375(3):247-260.
- [Google Scholar]
- From sad to happy to happier: Emotion regulation strategies used during a vacation. Ann. Tour. Res.. 2018;69:1-14.
- [Google Scholar]
- Multivariate Data Analysis (7 ed.). New York: Prentice Hall; 2010.
- Suboptimal health status and psychological symptoms among Chinese college students: a perspective of predictive, preventive and personalised health. EPMA J.. 2018;9(4):367-377.
- [Google Scholar]
- Exploring the relationship between work stress, years of experience and emotional competency using a sample of Australian mental health nurses. Psychiatr. Mental Health Nurs.. 2001;8(5):399-403.
- [Google Scholar]
- Work stress as a risk factor for cardiovascular disease. Curr. Cardiol. Rep.. 2015;17:74.
- [Google Scholar]
- Principles and Practice of Structural Equation Modeling. New York: Guilford Publications; 2015.
- Drivers and outcomes of green tourist attitudes and behavior: Sociodemographic moderating effects. Psychol. Market.. 2015;32(6):635-650.
- [Google Scholar]
- Relationship between stress-related psychosocial work factors and suboptimal health among Chinese medical staff: a cross-sectional study. BMJ Open. 2018;8(3):e018485.
- [Google Scholar]
- Association between lifestyle factors and suboptimal health status among Chinese college freshmen: A cross-sectional study. BMC Public Health. 2018;2(18):105.
- [Google Scholar]
- PTSD symptoms, hazardous drinking, and health functioning among U.S.OEF and OIF veterans presenting to primary care. J. Trauma. Stress. 2010;23(1):108-111.
- [Google Scholar]
- Psychometric evaluation of three versions of the Italian perceived stress scale. Curr. Psychol.. 2021;40(4):1884-1892.
- [Google Scholar]
- Predictors of tourists’ shopping behaviour: Examination of socio-demographic characteristics and trip typologies. J. Vacation Market.. 2004;19(4):308-319.
- [Google Scholar]
- Binge drinking and health-related quality of life: Do popular perceptions match reality? Am. J. Prev. Med.. 2004;26(3):230-233.
- [Google Scholar]
- Rural wellbeing tourism: Motivations and expectations. J. Hosp. Tour. Manage.. 2010;17(1):150-157.
- [Google Scholar]
- Family adventure tourism: Towards hedonic and eudaimonic wellbeing. Tour. Manage. Perspect.. 2021;39:100852.
- [Google Scholar]
- Understanding the value of tourism to seniors’ health and positive aging. Int. J. Environ. Res. Public Health. 2022;19:1476.
- [Google Scholar]
- Influence of tourists’ sociodemographic characteristics on their perception of destination personality and emotional experience of a city break destination. Int. J. Tour. Cities. 2021;7(1):200-223.
- [Google Scholar]
- Conducting and interpreting canonical correlation analysis in personality research: A user-friendly primer. J. Pers. Assess.. 2005;84(1):37-48.
- [Google Scholar]
- Tea drinking and the tastescapes of wellbeing in tourism. Tour. Geogr. 2020
- [CrossRef] [Google Scholar]
- Using Multivariate Statistics (6th ed.). 2014.
- Cardiovascular health in China: Low level vs high diversity. Lancet Regional Health-West. Pac.. 2020;3:100038.
- [Google Scholar]
- China suboptimal health cohort study: rationale, design and baseline characteristics. J. Transl. Med.. 2016;14(1):1-12.
- [Google Scholar]
- Association between ideal cardiovascular health metrics and suboptimal health status in Chinese population. Sci. Rep.. 2017;7(1)
- [Google Scholar]
- Wang, W., Tan, X. 2019. Suboptimal health status and cardiovascular deficits. In O. Golubnitschaja (Ed.), Flammer Syndrome: Advances in Predictive, Preventive and Personalised Medicine (Vol 11; pp. 287–315). Springer, Cham.
- Suboptimal health: A new health dimension for translational medicine. Clin. Transl. Med.. 2012;1(28):1-6.
- [Google Scholar]
- Wang, X., Zhong, Z., Balmer, L., Wang, W. (2021). Glycosylation profiling as a biomarker of suboptimal health status for chronic disease stratification. In G. Lauc, I. Trbojević-Akmačić (Eds.) The role of glycosylation in health and disease. Advances in experimental medicine and biology, vol 1325. Springer, Cham.
- The missing link between medical science knowledge and public awareness: implications for tourism and hospitality recovery after COVID-19. Eur. J. Manage. Bus. Econ.. 2021;30(2):230-242.
- [Google Scholar]
- COVID-19: potential effects on Chinese citizens’ lifestyle and travel. Tour. Rev.. 2021;76(1):74-87.
- [Google Scholar]
- Many brains are better than one: the importance of interdisciplinary studies on COVID-19 in and beyond tourism. Tour. Recreat. Res.. 2021;46(2):310-313.
- [Google Scholar]
- Tourism as a dementia treatment based on positive psychology. Tour. Manage.. 2022;92:104556.
- [Google Scholar]
- World Health Organization. 1946. Preamble to the Constitution of the World Health Organization as adopted by the International Health conference, New York, 19–22 June, 1946. New York: WHO.
- Prevalence and associated lifestyle factors of suboptimal health status among Chinese children using a multi-level model. Int. J. Environ. Res. Public Health. 2020;17(5):1497.
- [Google Scholar]
- Associations of environment and lifestyle factors with suboptimal health status: A population-based cross-sectional study in urban China. Global. Health. 2021;17(1):1-12.
- [Google Scholar]
- Association of suboptimal health status and cardiovascular risk factors in urban Chinese workers. J. Urban Health. 2012;89(2):329-338.
- [Google Scholar]
- Association of suboptimal health status with psychosocial stress, plasma cortisol and mRNA expression of glucocorticoid receptor α/β in lymphocyte. Stress. 2015;18(1):29-34.
- [Google Scholar]
- Development and evaluation of a questionnaire for measuring suboptimal health status in urban Chinese. J. Epidemiol.. 2009;19(6):333-341.
- [Google Scholar]
- Factor analysis of the COVID-19 perceived risk scale: A preliminary study. Death Stud.. 2022;46(5):1065-1072.
- [Google Scholar]
- The Burden of Alzheimer’s Disease Mortality in the United States, 1999–2018. J. Alzheimers Dis.. 2021;82(2):803-813.
- [Google Scholar]
- Afraid to travel after COVID-19? Self-protection, coping and resilience against pandemic ‘travel fear’. Tour. Manage.. 2021;83:104261.
- [Google Scholar]
- The role of trust in mitigating perceived threat, fear, and travel avoidance after a pandemic outbreak: A multigroup analysis. J. Travel Res.. 2022;61(3):582-1196.
- [Google Scholar]
- Rethinking the consequences of postmodern authenticity: the case of a World Cultural Heritage in Augmented Reality. Curr. Issues Tour. 2022
- [CrossRef] [Google Scholar]




