

Translate this page into:
The iron deficiency anemia in association to Helicobacter pylori infection in Najran city, Saudi Arabia
⁎Corresponding authors. mmubaraki@ksu.edu.sa (Murad A. Mubaraki),
-
Received: ,
Accepted: ,
This article was originally published by Elsevier and was migrated to Scientific Scholar after the change of Publisher.
Peer review under responsibility of King Saud University.
Abstract
Despite previous studies showing that Helicobacter pylori influences iron consumption, it is unknown what causes iron deficiency anemia in response to H. pylori infection. The goal of the study was to find out whether having an infection with H. pylori was linked to a drop-in serum iron level. Detection of H. pylori infection presented by serological test to detect titers of IgG and IgA in blood serum. The determination of iron serum level was performed by using biochemistry spectrophotometry test. Additionally, a full blood count was done to assess the haemoglobin concentration and establish whether the patient was anemic. Data analysis included descriptive statistics, Chi-square, and Mann–Whitney U test. Approximately 35% of the H. pylori group reported a low serum iron level against a 5% only in the control group. Also, the total bilirubin levels were 2.6-fold more among H. pylori positive cases than controls. H. pylori can cause a decrease in serum iron levels in infected individuals and eventually lead to iron deficiency anemia. Moreover, high total bilirubin levels are recorded among H. pylori-infected patients.
Keywords
Helicobacter pylori
Serum iron
Anemia
Iron deficiency anemia
Total bilirubin

1 Introduction
The World Health Organization claims that anemia, which affects a large section of the population, is a global health concern (WHO, 2008). Iron deficiency anemia (IDA) is known to be the most prevalent type of anemia with most IDA patients living in developing countries. IDA occurs in 2%–5% of adult men and postmenopausal women in the developed world, with blood loss from the gastrointestinal tract being the most common cause. Importantly, 15% of cases are considered unexplained IDA (Hershko and Camaschella, 2014). The relevance between Helicobacter pylori and IDA was first identified in 1991, as the patient with IDA displayed an improvement in blood parameters after the eradication of H. pylori (Demerdash et al., 2018; Nasif et al., 2021).
H. pylori is a gram negative spiral shaped bacterium that affect >50% of population mostly in developing countries (Ceylan et al., 2007). H. pylori infection can range from mild or asymptomatic gastritis to severe peptic ulcer; nevertheless, the complication of H. pylori infection is not frequent among children and adolescent in contrast to adults. In the absence of treatment, H. pylori could stay permanently, and it’s commonly being acquired during childhood (Kady et al., 2020; Parikh and Ahlawat, 2021).
The main explanation of the association between H. pylori and IDA remains unknown; however, there are certain causes could explain this correlation include: gastric bleeding caused by colonization of H. pylori, competing with the host for iron uptake, and the interference with iron absorption leading to increase iron wastage. In addition, some studies stated that there was a poor response of anemic patients to oral iron supplements with the presence of H. pylori infection (Kady et al., 2020; Monzón et al., 2013; Tseng et al., 2019; Hussain and Nisha, 2021).
According to Burns et al. (2017), the mouse model created is an effective tool for researching the neurologic, behavioural, and hematologic effects of the prevalent co-morbidity of IDA and H. pylori infection in humans.
In addition to IDA, Helicobacter pylori has been considered to cause reduction in the level of vitamin B12, this can be due to the alteration of absorption caused by the bacteria leading to its deficiency (Kadhim et al., 2018). Also, a study state that H. pylori account as a separated risk factor for blood bilirubin reduction, however, there is few studies regarding the relation between H. pylori and serum bilirubin (Mwafy and Afana, 2018; Zhao et al., 2019).
The aim of this study is to describe the association of IDA in response to H. pylori infection by comparing the level of iron. As well as comparison between the level of vitamin B12 and serum bilirubin among affected individuals.
2 Materials and methods
2.1 Study design, setting and participants
A retrospective case-control study was conducted by retrieving data of H. pylori positive cases (200 participants) and a group of H. pylori negative controls (200 participants) from King Khalid hospital in Najran Region of Saudi Arabia from January 2018 to December 2019. Exclusion criteria included the use of antibiotics, bismuth, proton pump inhibitor (PPI) and H2-receptor antagonist within 4 weeks. Moreover, patients with evident gastrointestinal cancer, hematologic disorders, who received iron supplementation for at least 30 days, received erythropoietin injection, those with overt/occult gastrointestinal bleeding, with malnutrition, a history of gastrectomy, and those with recent hospitalization due to acute illnesses were also excluded.
2.2 Data collection
Patients were classified as having H. pylori infection when patients are positive for H. pylori IgG and IgA serological test. Semiquantitative determination of Ig-classes antibody of H. pylori in human serum, using a disposable device applied on the CHORUS instrument manufactured by DIESSE- Italy. The test follows the role of ELISA (Enzyme-linked Immunosorbent Assay) principle.
Collected blood samples were used to analyze the CBC parameters, white blood cells (WBC), red blood cells (RBC), hemoglobin (Hb), hematocrit (Hct), Mean Cell Volume (MCV), Mean Cell Hemoglobin (MCH), Mean Cell Hemoglobin Concentration (MCHC), Red Cell Distribution Width (RDW), and platelet count (Plt). Sysmex KX-21 N- Japan automated hematology analyzer was used to obtain the results.
Iron is one of the most important elements to produce healthy RBCs. It is almost half part of hemoglobin. COBAS 6000 analyzers automatically calculate the analytic concentration in each sample. The normal value of iron among males was 10.6–28.3 μmol/L while in females it was 6.6–26.0 μmol/L.
Vitamin B12 is necessary for the formation of normal RBCs, DNA synthesis, and tissue and cellular repair. A deficiency in vitamin B12 can cause macrocytic anemia (megaloblastic anemia). The characterization of this condition is by the production of fewer RBCs, but larger in size, called macrocytes. Cobas e 601- Roche- Switzerland analyzer was used to obtain this test. The technique tests were utilizing serum binding proteins or partially purified intrinsic factors to estimate the degrees of vitB12. A reference range of 180–914 pg/mL was set according to laboratory policy.
Total bilirubin level measurement has a major role in the diagnosis and treatment of hemolytic anemia and liver disorders. The heme protein which formed the hemoglobin is metabolized to form the bilirubin. A normal range of 3–17 μmol/L was used according to the local laboratory policy.
Ethical approval was granted by the Institutional Review Board IRB of the General Directorate of Health Affairs Najran, Saudi Arabia (KACST, KSA: H-l1-N-081). Informed consent was obtained from each patient involved in this study.
2.3 Statistical analysis
All values are shown as mean ± standard error of the mean as indicated. Differences between groups were analyzed using the nonparametric Mann–Whitney U test performed using GraphPad Prism 9.0 software.
3 Results
3.1 Demographic characteristics and age distribution of participants
The difference regarding the gender of participants was taken into consideration as the recruited numbers of females and males were equally distributed among the two groups (100 females and 100 males participated in each group). To examine the correlation between the age of the participants and the prevalence of H. pylori infection, the 400 participants were distributed into three groups according to their age in year (<35, 35–44 and >44) as shown in Table.1. The data revealed that 66.5% of the participants were in the youngest age group of <35 years followed by the age of 35–44 years with 19.5%, and the age group that participated the least was the age of >44 years with only 14%. *Denote the percentage of each age group who were partcipated in the study, while the bold numbers represent the percentage of H. pylori cases in each age group.
Age group
yearFemale n
(%)Male n
(%)Grand Total N
(%)
<35
146 (73%)*
120 (60%)*
266 (66.5%)*
Cases
56 (38%)
45 (37%)
101 (38%)
Control
90
75
165
35–44
30 (15%)*
48 (24%)*
78 (19.5%)*
Cases
22 (73%)
29 (60%)
51 (65%)
Control
8
19
27
>44
24 (12%)*
32 (16%)*
56 (14%)*
Cases
22 (91%)
26 (81%)
48 (86%)
Control
2
6
8
Grand Total
200
200
400
3.2 H. pylori cases have more risk to develop iron deficiency anemia
To investigate, the correlation between the H. pylori infection and iron deficiency anemia, results for Hb concentration and serum iron levels in H. pylori positive cases and H. pylori negative controls were compared. Overall, the results show that the Hb concentration of H. pylori positive cases were onefold lower than H. pylori negative controls (P-value <0.0001) (Fig. 1A). More remarkably, the serum iron levels in H. pylori positive cases were 1.3-fold lower than the negative controls (P-value <0.0001) (Fig. 1B). The serum iron levels collected from all the participants of both groups were assessed individually by the hematologist according to the following reference ranges: Males 10.6–28.3 μmol/L, Females 6.6–26.0 μmol/L. Interestingly, 35% of H. pylori positive cases had low iron levels (70 out of 200) while in H. pylori negative controls, only 5% had low iron levels (10 out of 200). This indicates that H. pylori infection increases the risk of iron deficiency to individuals by 7-fold when comparing H. pylori positive cases with the negative controls (Table 2).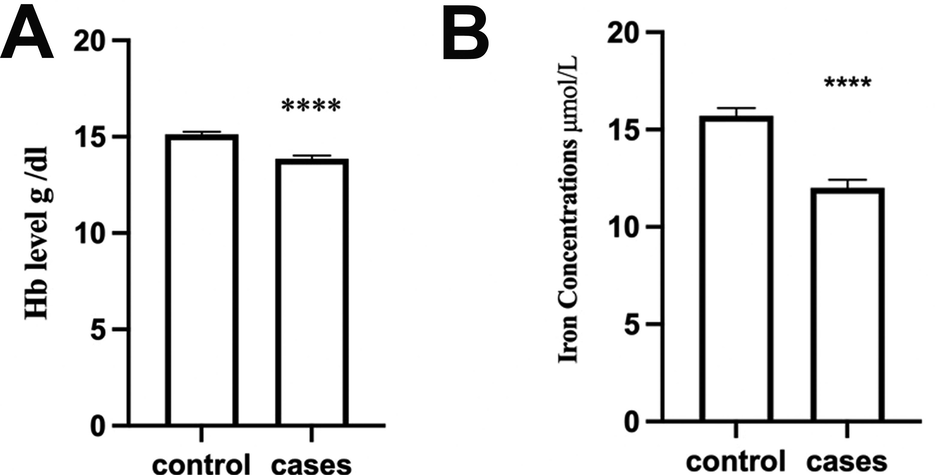
Levels of Hb concentration and serum iron among H. pylori negative control and H. pylori positive cases. The data represents the mean ± SEM in each group. The asterisks indicate P-value <0.0001.
Cases N (%)
Control N
(%)Chi-Square
P-Value
Iron
Low
70 (35)
10 (5)
56.25
0.05
Normal
130 (65)
190 (95)
3.3 H. pylori infection has no effect on vitamin B12
To examine the relationship between the H. pylori infection and the deficiency of vitamin B12, the levels for the vitamin B12 in H. pylori positive cases and H. pylori negative controls were compared. As shown in Fig. 2A, there was no significant difference in vitamin B12 between H. pylori positive cases and H. pylori negative controls. Moreover, the percentage of individual cases with low vitamin B12 was insignificant compared to controls, 17% in cases (35 out of 200) and 20% (40 out of 200) respectively.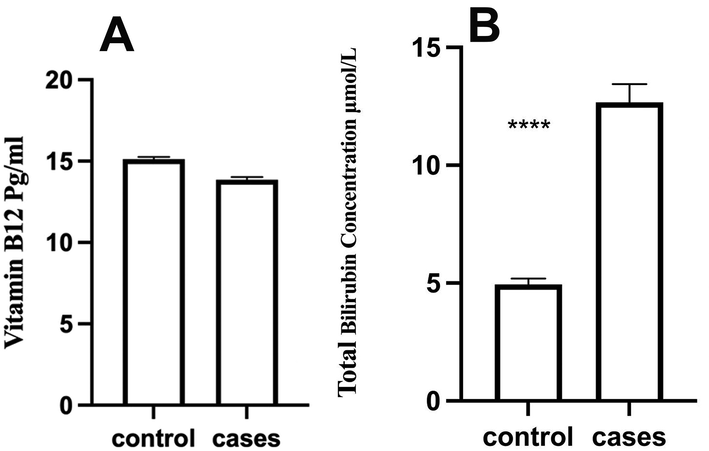
The Level of vitamin B12 (A) and total bilirubin (B) among H. pylori negative control and H. pylori positive cases. The data represents the mean ± SEM in each group. The asterisks indicate P value <0.0001.
3.4 H. pylori cases showed increased levels of total bilirubin
To examine if H. pylori have any effect on liver function and/or the rate of red blood cells breakdown, levels of total bilirubin were compared in H. pylori positive cases and H. pylori negative controls. Interestingly, H. pylori positive cases showed 2.6-fold increase in the total bilirubin compared to H. pylori negative controls (P-value <0.0001) Fig. 2B. Furthermore, the percentage of individuals with high total bilirubin were significantly more in cases compared to controls, 15.5% in cases (31 out of 200) and 3% (6 out of 200) respectively.
4 Discussion
H. pylori is a bacterium that causes gastritis, and it is very common among the population especially in developing countries (Mitchell and Katelaris, 2016). Various studies performed in counties such as China, Palestine, Ethiopia, and Spain associated H. pylori infection with IDA although the mechanism of this association is unclear (Monzón et al., 2013; Kibru et al., 2014; Hou et al., 2019; Mwafy and Afana, 2018; Haile and Timerga, 2021). Moreover, some studies correlated H. pylori infection with vitamin B12 deficiency and found that treating H. pylori infection had restored the vitamin B12 to normal levels (Sarari et al., 2008; Humeida, 2017; Mwafy and Afana, 2018).
In our retrospective case-control study, we included data from 200 H. pylori positive participants and 200 H. pylori negative control participants from the regional laboratory in the Najran Region. Since females are more prone to IDA due to blood loss in the menstrual cycle compared to males, our study included equal numbers of males and females in both cases and controls groups. Our study confirms the association between H. pylori infection and iron deficiency anemia. Both Hb concentration and serum iron levels were significantly lower in H. pylori positive cases compared to controls and the prevalence of iron deficiency was seven times more in H. pylori positive cases compared to controls. This finding is in line with a recent study performed in Ethiopia as well as other studies performed in Karachi (Zuberi et al., 2007), Palestine (Mwafy and Afana, 2018), Egypt (Rahman et al., 2019). Nevertheless, one study conducted in Dhaka, Bangladesh found that H. pylori was significantly associated with iron deficiency but not with anemia (Rahman et al., 2020). Moreover, another study has contradicted the association of H. pylori with IDA in males with normal gastrointestinal tract endoscopy results (Nasif et al., 2021). The contradiction between these studies and ours could be a result of differences in the sample size and methodology. Though the mechanism of association is uncertain, it has been suggested that colonization of the stomach by H. pylori disturbs the gastric mucosa which may result in a reduction of iron absorption secondary to chronic gastritis and hypochlorhydria (Monzón et al., 2013). Other mechanisms of anemia include blood loss due to chronic erosive gastritis and consumption of iron by H. pylori (Haile and Timerga, 2021).
Surprisingly, our study shows no correlation between H. pylori infection and vitamin B12 deficiency which contradicts other studies conducted in other countries (Sarari et al., 2008; Humeida, 2017; Mwafy and Afana, 2018; Haile and Timerga, 2021). This contradiction could be due to dissimilarities in the diet source of vitamin B12 among different populations or due to variation in the sample size and methodology. Interestingly, our study showed for the first time that H. pylori infection is associated with higher total bilirubin levels compared to controls as the H. pylori positive cases were 2.6-fold more than controls. The mechanism of this association is unknown; however, it has been reported that H. pylori can be transmitted to the liver through the portal vein or through the bile duct which can result in hepatobiliary diseases (Nilsson et al., 2000; Pellicano et al., 2008).
There aren't enough studies on the link between H. pylori infection and IDA in the Saudi population, and the most recent study had 79 patients (Nasif et al., 2021), whereas our sample size is 400. Additionally, this study shed the light on the association between H. pylori infection and high total bilirubin levels which worth to be investigating further to find the mechanism of this association whether it is due to early break down of red blood cells or due to hepatobiliary diseases caused by H. pylori infection. On the other hand, this study has limitations due to its cross-sectional nature as it does not display a cause- effect relationship between variables. It would be interesting to investigate the mechanism of iron deficiency by examining the effect of restoring iron in H. pylori positive individuals with iron supplements in one group and with iron infusion in another group to assess if H. pylori affect the absorbance of iron or the reason of iron deficiency is due to blood loss. Moreover, the main contributors to the current study were the younger population. Hence, one should be cautious in interpreting these results in the context of age and more studies should be conducted to examine the older population.
5 Conclusions
This study showed a significant reduction in Hb-concentration and iron levels in H. pylori-infected patients compared to controls. Interestingly, in our study vitamin B12 levels show no association with H. pylori infection. Furthermore, H. pylori-infected patients showed higher total bilirubin levels which may be worth being investigated further in a large longitudinal community-based study. This study emphasizes the importance of eradication of H. pylori from infected patients since its negative effect has been confirmed to be beyond the stomach. To fully comprehend the various relationships between IDA and H. pylori infection, more research is necessary.
Acknowledgment
This study was supported by Princess Nourah bint Abdulrahman University Researchers Supporting Project number (PNURSP2022R96), Princess Nourah bint Abdulrahman University, Riyadh, Saudi Arabia.
Declaration of Competing Interest
The authors declare that they have no known competing financial interests or personal relationships that could have appeared to influence the work reported in this paper.
References
- Helicobacter pylori infection and low dietary iron alter behavior, induce iron deficiency anemia, and modulate hippocampal gene expression in female C57BL/6 mice. PLoS ONE. 2017;12(3):e0173108.
- [Google Scholar]
- Prevalence of Helicobacter pylori in children and their family members in a district in Turkey. J. Health Popul. Nutr.. 2007;25(4):422.
- [Google Scholar]
- Helicobacter pylori associated to unexplained or refractory iron deficiency anemia: an Egyptian single-center experience. Hematol. Transfus Cell Ther.. 2018;40(3):219-225.
- [Google Scholar]
- Evaluation of hematological parameters of Helicobacter pylori-infected adult patients at Southern Ethiopia: A comparative cross-sectional study. J. Blood Med.. 2021;12:77-84.
- [Google Scholar]
- How I treat unexplained refractory iron deficiency anemia. Blood. 2014;123(3):326-333.
- [Google Scholar]
- Association of active Helicobacter pylori infection and anemia in elderly males. BMC Inf. Dis.. 2019;19(1):228.
- [Google Scholar]
- Association of Helicobacter pylori infection and vitamin B12 level among sudanese patients. IOSR J Dent Med Sci. 2017;16(03):12-14.
- [Google Scholar]
- A study on prevalence, type and severity of anemia in Helicobacter Pylori infection with respect to RBC parameters in a tertiary care hospital. Saudi J. Pathol. Microbiol.. 2021;6(3):100-104.
- [Google Scholar]
- Vitamin B12 deficiency in Helicobacter pylori infected patients. OALib. 2018;5(03):1-4.
- [Google Scholar]
- Burden of Helicobacter pylori infections and associated risk factors among cases of iron deficiency anaemia in Egypt. Microbiol Res J Int. 2020;19:80-91.
- [Google Scholar]
- Helicobacter pylori infection and its association with anemia among adult dyspeptic patients attending Butajira Hospital, Ethiopia. BMC Infect. Dis.. 2014;14:656.
- [Google Scholar]
- Epidemiology, clinical impacts and current clinical management of Helicobacter pylori infection. Med. J. Aust.. 2016;204(10):376-380.
- [Google Scholar]
- Helicobacter pylori infection as a cause of iron deficiency anaemia of unknown origin. World J. Gastroenterol.. 2013;19(26):4166-4171.
- [Google Scholar]
- Hematological parameters, serum iron and vitamin B12 levels in hospitalized Palestinian adult patients infected with Helicobacter pylori: a case-control study. Hematol. Transfus Cell Ther.. 2018;40(2):160-165.
- [Google Scholar]
- Impact of Helicobacter pylori on hematological parameters among Saudi population. Saudi Med. J.. 2021;42(6):643-648.
- [Google Scholar]
- Identification of Helicobacter pylori and other Helicobacter species by PCR, hybridization, and partial DNA sequencing in human liver samples from patients with primary sclerosing cholangitis or primary biliary cirrhosis. J. Clin. Microbiol.. 2000;38(3):1072-1076.
- [Google Scholar]
- Parikh, N.S., Ahlawat, R. (2021). Helicobacter Pylori. In StatPearls. StatPearls Publishing. PMID: 30480966.
- Helicobacter species and liver diseases: association or causation? Lancet Infect Dis.. 2008;8(4):254-260.
- [Google Scholar]
- Association between Helicobacter Pylori infection and iron deficiency anemia: A cross sectional study. J. Bangladesh Coll. Phys. Surg.. 2020;38(2):68-78.
- [Google Scholar]
- Helicobacter pylori and its hematological effect. Egypt J. Intern. Med.. 2019;31(3):332-342.
- [Google Scholar]
- Helicobacter pylori, a causative agent of vitamin B12 deficiency. J. Infect. Dev. Ctries. 2008;2(5):346-349.
- [Google Scholar]
- Effect of Helicobacter pylori treatment on unexplained iron deficiency anemia. The Perm J.. 2019;23:18-195.
- [Google Scholar]
- WHO (2008). Anaemia. World Health Organization. https://www.who.int/data/nutrition/nlis/info/anaemia.
- Helicobacter pylori infection as a risk factor for serum bilirubin change and less favourable lipid profiles: a hospital-based health examination survey. BMC Inf. Dis.. 2019;19(1):157.
- [Google Scholar]
- Hemogolbin, ferritin, vitamin B12 and halicobacter pylori infection: a study in patients who underwent upper gi endoscopy at civil hospital karachi. J. Coll. Phys. Surg.-Pakistan. 2007;17(9):546-549.
- [Google Scholar]




