

Translate this page into:
The effect of aerobic exercise combined with metformin on ischemic cerebral infarction and its effect on the molecular level of SOD
⁎Corresponding author at: Department of OR, No. 1 Hospital Branch 2 of Jilin University, Jilin, Changchun, China. jinweiweijlu@163.com (Weiwei Jin)
-
Received: ,
Accepted: ,
This article was originally published by Elsevier and was migrated to Scientific Scholar after the change of Publisher.
Peer review under responsibility of King Saud University.
Abstract
To explore the therapeutic effect of aerobic exercise combined with metformin on ischemic cerebral infarction (ICI) and its effect on the molecular level, 100 patients with ICI who were treated in our hospital from January 2014 to December 2018 were selected as the study objects. According to the principle of random grouping, they were divided into the control group (50 cases, treated by metformin alone) and the observation group (50 cases, treated by aerobic exercise combined with metformin). Before and after treatment, the relevant indicators of the two groups were collected and analyzed statistically. The results showed that the total effective rate of the observation group was significantly higher than that of the control group (P < 0.05); the whole blood viscosity, plasma viscosity, and erythrocyte electrophoresis of the two groups were significantly lower after treatment (P < 0.05), and the observation group was significantly lower than the control group (P < 0.05). The level of superoxide dismutase (SOD) and lipid peroxide (LPO) in the two groups were compared and analyzed. It was found that the SOD level in the observation group was significantly higher than that in the control group (P < 0.05), and the LPO level in the observation group was significantly lower than that in the control group (P < 0.05). Therefore, through this study, it is found that the combination of aerobic exercise and metformin can significantly improve the hemorheological indexes of patients with ICI, and can promote the activity of SOD. Moreover, it can significantly reduce the level of LPO, which provides experimental basis for the treatment of patients with ICI in the late clinical stage.
Keywords
Metformin
Aerobic exercise
Hemorheology
SOD
LPO

1 Introduction
Ischemic cerebral infarction (ICI) also called ischemic cerebral stroke, it refers to local cerebral tissue ischemic necrosis of cerebral tissue ischemia and anoxia caused by cerebral local blood-supply dysfunction. Incidence rate accounts for 70% in cerebral stroke (Zhang et al., 2016), it is a common clinical disease with high death rate and disability rate. It usually occurs in middle-aged and old people, severely affecting people’s health and life quality, which bring heavy burden to family and whole society of patients.
With the development of economy and society of China, the trend of population aging is more obvious. Incidence rate of ICI is increasing year by year (Tang et al., 2017). Risk factors of cerebral infarction include hyperglycemia, hypertension, hyperlipidemia and arrhythmia etc. The clinical manifestations include cerebral edema, coma, hemiplegia, linguistic disorder and diagnosis (Chen et al., 2015).
Currently, the treatment of cerebral infarction is mainly thrombolysis, anticoagulation and decompression etc. (Wang, 2015). Metformin is the first-line drug to treat type II diabetes, which can effectively lower blood glucose. Epidemiology investigation shows that the rate and degree of cerebral infarction patients of diabetes patients by metformin all significantly decreased. Therefore, metformin has the possibility of becoming new drug for treating ICI (Lv et al., 2015).
Aerobic exercise is an exercise method of moderate and strong intensity controlled by aerobic metabolism. It has been applied into rehabilitation treatment of cerebral stroke. Linder et al. (Linder et al., 2019) believed that strengthening aerobic exercise training could promote the exercise recovery after stroke as the central nervous system was optimized (Linder et al., 2019). SOD and LPO in blood separately reflect ability of body cleaning free radical and level of oxygen free radical in vivo, which can be markers of recovery level of cerebral infarction and recovery ability, also can be a kind of reference for prognosis (Wang, 2017).
To explore the effect of aerobic exercise combined with metformin on the treatment of ICI and its molecular level, 100 patients with ICI were divided into the control group and the observation group. The therapeutic effect, hemorheology, SOD, and LPO levels of the two groups were compared. The innovation of this paper lies in verifying the clinical effect of aerobic exercise combined with metformin, and analyze its role at the molecular level, thereby providing guidance for the clinical treatment of ICI.
2 Materials and methods
2.1 General data
This clinical study regarded ICI patients as study subjects. All cases were 100 cases in our hospital from January 2014 to December 2018. Inclusive criteria concerned first, according to Diagnosis criteria of ischemic cerebral injury after cerebral hemorrhage formulated by The Fourth National Conference on the diagnosis of cerebrovascular disease academic standards, it was diagnosed as ICI. Second, it had been demonstrated by medical iconography data of computed tomography (CT) and magnetic resonance imaging (MRI). Third, patients who had no concurrent severe diseases in heart, lung, liver and kidney. Fourth, patients were in informed state. Fifth, nervous functional defects scoring was from 16 to 30.
Exclusive criteria concerned first, patients who had severe diseases in heart, lung, liver, kidney and tumor; second, patients who had psychological diseases and senile dementia, they not cooperated with disease treatment. Third, patients who not agreed to participates in study. There were 62 males and 38 females. Ages were from 52 to 76 years. Mean age was 64.1 ± 8.1 years. Cerebral infarction location: there were 52 cases in basal ganglia region, 25 cases with multiple onset, 13 cases in centrum semiovale and 10 cases in epencephalon. All approved by ethics committee and informed consent. Study patients in this study were randomly divided into the control group and the observation group by using computer software, each group 50 cases. There were 32 males and 18 females in the control group. Ages were from 52 to 75 years. Mean age was 63.9 ± 8.0 years. There were 30 males and 20 females in the observation group. Ages were from 53 to 76 years. Mean age was 64.2 ± 8.2 years. Compared demography data, disease history, infarction location and degree of patients in two groups, there were no obvious differences (P > 0.05).
2.2 Treatment methods
The control group: according to conditions of patients, they were given anticoagulation, blood pressure-lowering, lipid-lowering and metformin treatment. Metformin hydrochloride tablets (trade name: Glucophage, specification: 0.5gx20 of one tablet, approval number: SFDA approval numberH20023370, production enterprises: Sino-US Shanghai Squibb pharmaceutical CO., Ltd), oral administration once one day. Twice one day in the morning and evening according to meal. The observation group: it given aerobic exercise rehabilitation on the basis of the control group. MOTOmedviva2 threadmill training in seat once one day was adopted. Patients given traction of lower limbs and activity of knee and hip joint before exercises. Motion resistance was it was difficult to kick for patients. The time was 20 min. The they kicked bicycle for 3 min, finally tuina for 3 min. Course of patients in two groups was one month.
2.3 Observation indexes
2.3.1 Hemorheology indexes
3 ml venous blood in empty stomach in the morning before and after treatment was extracted. LIANG-100 microcomputer system used to record blood plasma viscosity spontaneously. WBHSV (Whole Blood High Shear Viscosity), WBLSV (Whole Blood Low Shear Viscosity), plasma visibility, and erythrocyte electrophoresis were compared between the two groups. CEU—DYN 1700 globulimeter from America Abbott company used to record HCT (hematocrit).
2.3.2 Blood SOD and LPO level
3 ml venous blood in empty stomach in the morning before and after treatment was extracted. They were given 3000 rpm centrifugation for 10 min. Serum was fetched. TB enzyme method used to detect Serum LPO level. Xanthine chloridize enzyme method to detect serum SOD level.
2.3.3 Bone metabolic indexes
5 ml venous blood before and after treatment was extracted. They were given 3000 rpm centrifugation for 10 min. 0.5–1 ml supernatant was fetched for storage to be detected. Biochemical analyzer used to detect serum calcium ion, phosphorus and Cr. Instrument company was America Beckman company. Urine was collected in two time points were collected. Calcium ion of urine was detected. ELISA (Enzyme Linked Immunosorbent Assay) method used to detect serum BGP (Bone Gla-Protein) and NTx (N-telopeptide of typeⅠcollagen). Instrument production company was America BIORAD. Kits bought from Beijing Yinghua company.
2.3.4 Effects criteria
First, complete recovery: signs of neurosis disappeared completely. The consciousness recovered. Patients can take care of themselves in daily life and work normally; obvious effects: nervous functional defects scoring was 21 points or over; patients can take care of themselves in daily life; validity: nervous functional defects scoring was 8 points or over, and less than 21 points, patients can walk under the help of walking stick; invalidity: nervous functional defects scoring less than 8 points, the symptoms aggravated or had no improvement.
2.4 Statistical methods
SPSS22.0 used to do statistical analysis for data in this study. Measurement data were represented as mean ± SD. Enumeration data were represented as % and done with X2 test as well as t test. Statistical significance was assumed at p < 0.05.
3 Results
3.1 Comparison of effects of patients in two groups
Recovery rate of patients in observation group significantly higher than the control group (P < 0.05), the total effective rate significantly higher than the control group (P < 0.05). It is shown in the Table 1.
Group
n
Recovery
Obvious effects
Validity
Invalidity
Effective rate
The observation group
50
13(26.0%)
22(44.0%)
11(22.0%)
4(8.0%)
46(92.0%)
The control group
50
5(10.0%)
15(30.0%)
18(36.0%)
12(24.0%)
38(76.0%)
χ2
4.336
2.102
2.380
4.762
4.762
P
0.037
0.147
0.123
0.029
0.029
3.2 Comparison of hemorheology of patients in two groups before and after treatment
Whole blood viscosity, plasma viscosity and erythrocyte electrophoresis of patients in two groups after treatment significantly decreased (P < 0.05). HCT in the observation group after treatment significantly decreased (P < 0.05); the observation group had no obvious decrease (P > 0.05); after treatment, Whole blood viscosity, plasma viscosity, erythrocyte electrophoresis and HCT significantly lower than the control group (P < 0.05). It is shown in the Table 2 and Fig. 1. Note: “*” means there were significant differences before treatment (P < 0.05); “#” means there were significant differences compared with the control group (P < 0.05).
Group
Time points
WBLSV (mPa·s)
WBHSV (mPa·s)
Plasma viscosity (mPa·s)
Erythrocyte electrophoresis
HCT
The observation group
Before treatment
9.14 ± 2.12
7.61 ± 0.85
2.03 ± 0.31
21.02 ± 2.21
0.50 ± 0.04
After treatment
6.36 ± 1.91*#
5.43 ± 0.83*#
1.41 ± 0.24*#
16.41 ± 2.04*#
0.46 ± 0.05*#
The control group
Before treatment
9.16 ± 2.14
7.58 ± 0.82
2.06 ± 0.35
21.10 ± 2.17
0.49 ± 0.04
After treatment
7.69 ± 1.95*
6.34 ± 0.80*
1.62 ± 0.27*
18.83 ± 1.97*
0.48 ± 0.05
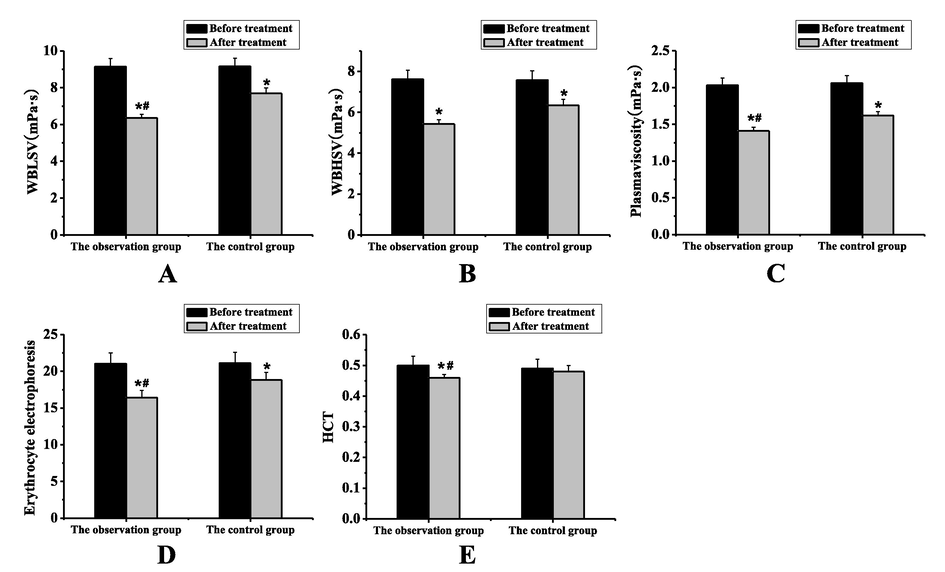
Comparison of hemorheology of patients in two groups before and after treatment (A: WBLSV; B: WBHSV; C: Plasma viscosity; D: erythrocyte electrophoresis; E: HCT; “*” means there were significant differences before treatment (P < 0.05); “#” means there were significant differences compared with the control group (P < 0.05)).
3.3 Comparison of SOD and LPO levels of patients in two groups
SOD of patients in the observation group after treatment significantly higher than the control group; LPO decreased (P < 0.05). LPO of patients in the observation group significantly lower than the control group (P < 0.05). It is shown in the Table 3 and Fig. 2. Note: “*” means there were significant differences before treatment (P < 0.05); “#” means there were significant differences compared with the control group (P < 0.05).
Group
Time points
SOD (U/L)
LPO (μmol/L)
The observation group
Before treatment
665.12 ± 43.21
5.79 ± 0.74
After treatment
996.41 ± 42.04*#
4.56 ± 0.75*#
The control group
Before treatment
661.10 ± 42.17
5.74 ± 0.78
After treatment
768.83 ± 1.97*
5.08 ± 0.65*
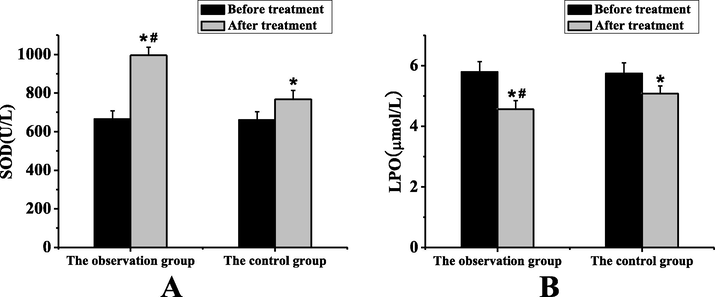
Comparison of SOD and LPO levels of patients in two groups of SOD and LPO levels of patients in two groups (“*” means there were significant differences before treatment (P < 0.05); “#” means there were significant differences compared with the control group (P < 0.05)).
4 Discussion
ICI refers to ischemic necrosis caused by cerebral local blood-supply dysfunction, further inducing a series of symptoms of nervous functional defects scoring (Cui et al., 2015). The mechanism of ICI has cerebral atherosclerosis, hyperlipidemia and hyperglycemia etc. They can be divided into main types including cerebral thrombosis, cerebral embolism and lacunar infarction (Sahara et al., 2016). With the development of society, progress of urbanization and development of population aging, incidence rate of cerebral infarction is becoming more and more high, it has become the second great disease in death rate (Yang, 2015). At present, treatment of ischemic infarction is early drug thrombolysis treatment with later rehabilitation (Shi et al., 2015). Drug treatment is mainly rt-PA (recombinant tissue plasminogen activator), it is the only drug used for cerebral infarction which has been approved by FDA (Food and Drug Administration). Therapeutic window is narrow, which needs to be used within 6 h after incidence (Tan and Wu, 2016). Metformin as one of first-line for treating diabetes. During application process, it has decreased function for incidence rate of cerebral infarction and severity (Luo et al., 2017). In multiple animal experiments, metformin reflects its neurological protection for rats with cerebral infarction and it can decrease infarction area, lower apoptosis of cerebral cells, improve blood brain barrier function after ischemia and promote recovery of nerve function and tissue recovery (Karimipour et al., 2018). Its function and mechanism are to promote changes of polarized state of microglia or macrophage cells by activating AMPK (Adenosine 5‘-monophosphate -activated protein kinase). It can lower inflammatory reactions, relieve the damage of inflammatory factors on blood brain barrier, promote generation of vessels and neurological cells, enhance nerve recovery, improve oxidative stress reaction level and protect nerve cells. Aerobic exercise can improve heart and lung function of patients, decrease muscular atrophy, improve oxygen-supply ability, promote recovery of infarction region by exercises, it has been widely applied in rehabilitation of cerebral infarction patients.
The recovery rate of patients in the observation group significantly higher than the control group (P<0.05). The total effective rate significantly higher than the control group (P<0.05). It shows that effects of aerobic exercise and metformin is more accurate on ICI. Whole blood viscosity, plasma viscosity and erythrocyte electrophoresis of patients in two groups after treatment significantly decrease (P < 0.05). HCT in the observation group after treatment significantly decrease (P < 0.05); after treatment, Whole blood viscosity, plasma viscosity, erythrocyte electrophoresis and HCT significantly lower than the control group (P < 0.05). It shows that aerobic exercise and metformin can more effectively lower hemorheology indexes, it may related to aerobic exercise can reduce high HCT caused by anoxia, promote oxidation metabolic rate, increase intracellular ATP (Adenosine Triphosphate) level, recover membrane function of erythrocyte and deformability and lower blood viscosity, thus improving cerebral blood-supply and promote recovery of infarction region (Cai et al., 2018; Li, 2014). SOD of patients in the two groups after treatment significantly higher than before treatment; LPO level significantly decreases (p < 0.05); SOD level of patients in the observation group after treatment significantly higher than the control group, LPO significantly decrease (P < 0.05). It shows that two treatments can effectively promote SOD level, improve clean ability of body on oxygen free radical, lower injury of hyperoxide on cellular membrane of nerve cells and mitochondrial membrane. Aerobic exercise and metformin can more effectively play this effect. The study of Yuan et al. (Yuan et al., 2019) showed that metformin can inhibit nerve aging and reduce infarct area (Yuan et al., 2019), which is consistent with the results of this study.
In conclusion, results of this study show that aerobic exercise and metformin may more effectively treat ICI, lower blood viscosity, improve blood oxygen supply in infarction region, significantly promote SOD level and lower free radical level, thereby enhancing nerve recovery and function recovery. However, the samples in this study is relatively less. The more accurate conclusion needs larger sample and more evidence to be demonstrated.
Declaration of Competing Interest
The authors declare that they have no known competing financial interests or personal relationships that could have appeared to influence the work reported in this paper.
References
- An antioxidant role by minocycline via enhancing the activation of LKB1/AMPK signaling in the process of cerebral ischemia injury. Curr. Mol. Med.. 2018;18(3):142-151.
- [Google Scholar]
- Analysis of risk factors of senile hemorrhagic cerebral infarction. China Public Health. 2015;31(3):359-361.
- [Google Scholar]
- Application of repeated transcranial stimulation in cerebral infarction patients[J] Chinese Journal of Rehabilitation Medicine. 2015;30(12):1301-1305.
- [Google Scholar]
- Pre-treatment with metformin in comparison with post-treatment reduces cerebral ischemia reperfusion induced injuries in rats. Bull. Emerg. Trauma. 2018;6(2):115-121.
- [Google Scholar]
- Influences of Mailuoning and high oxygen in treatment of hemorrheology of acute cerebral infarction and its effects observation. Nei Mongol J. Tradition. Chin. Med.. 2014;33(22):41-42.
- [Google Scholar]
- Forced, not voluntary, aerobic exercise enhances motor recovery in persons with chronic stroke. Neurorehabil. Neural Repair. 2019;33(8):681-690.
- [Google Scholar]
- Influences on cognition of metforminfor acute ischemic cerebral stroke. Clin. Educ. General Practice. 2017;15(4):445-446.
- [Google Scholar]
- Progress of cerebral protection and mechanism of metforminfor ischemic cerebral storke. Stroke Nervous Dis.. 2015;5:317-319.
- [Google Scholar]
- Cerebral infarction and transient ischemic attack. Nihon Rinsho Japanese J. Clin. Med.. 2016;74(4):666.
- [Google Scholar]
- Observation on recent effects of urinarykallid and rt-PA in treatment of super-early cerebral infarction. Beijing Med. J.. 2015;37(5):498-499.
- [Google Scholar]
- Efficacy and safety of rt-PA intravenous thrombolysis in the treatment of acute ischemic stroke with hyperdense middle cerebral artery sign: a systematic review. Chin. J. Contemporary Neurol. Neurosurg.. 2016;16(1):8-15.
- [Google Scholar]
- Metformin ameliorates sepsis-induced brain injury by inhibiting apoptosis, oxidative stress and neuroinflammation via the PI3K/Akt signaling pathway. Oncotarget. 2017;8(58):97977-97989.
- [Google Scholar]
- Effect of gangliosides combined with hyperbaric oxygenation on neural functional recovery and oxidative stress injury after cerebral infarction intervention. J. Hainan Med. Univ.. 2017;23(14):133-136.
- [Google Scholar]
- Influences of tracking mode nursing intervention for life quality of cerebral stroke patients. Shanxi Med. J.. 2015;13:1572-1574.
- [Google Scholar]
- Metformin reduces neuronal damage and promotes neuroblast proliferation and differentiation in a cerebral ischemia/reperfusion rat model. NeuroReport. 2019;30(3):1.
- [Google Scholar]
- Observation on effects of behavior nursing for exercise function recovery of cerebral infarction patients. J. Clin. Med. Pract.. 2016;20(14):147-148.
- [Google Scholar]




