

Translate this page into:
Rapid measurement of lumbosacral spine-pelvic sagittal balance parameters using electronic device
⁎Corresponding authors. yyj2019eygk@sina.com (Yijun Yang), zhh1968jzwk@sina.com (Haihong Zhang)
-
Received: ,
Accepted: ,
This article was originally published by Elsevier and was migrated to Scientific Scholar after the change of Publisher.
Abstract
Background
Picture Archiving and Communication Systems (PACS) is the gold standard for the measurement of spinal parameters. The aim of this study is to evaluate the practical value of using an iPhone to rapidly measure lumbosacral spine-pelvic sagittal parameters, and compared the measurement time and accuracy between iPhone and PACS.
Methods
The study group consisted of 50 patients. They were examined with a lateral x-ray of the whole spine in a standard standing position, as well as by three-dimensional CT scan of the lumbosacral area from January to September 2016. An iPhone was employed to take and observe pictures in order to measure the extent of lumbar lordosis (LL), pelvic tilt (PT), and sacral slope (SS). We compared the results with those obtained with PACS, and analyzed the reliability and measurement errors between the two acquisition methods.
Results
The average measurement values obtained with PACS were as follows: (LL): 53.56 ± 15.76°, (PT): 12.60 ± 5.15°, (SS): 42.16 ± 13.29°. The average measurement values obtained by iPhone were as follows: LL: 52.20 ± 14.46°, PT: 12.48 ± 5.39°, SS: 12.48 ± 5.39°. There was no statistical significance difference found between the values obtained using the two methods, P > 0.05. The two methods of measurement of intra-class correlation coefficients (ICCs) were 0.938(De-LL), 0.812(De-PT) and 0.946(De-SS). There was no statistically significant difference in the deviation between the two measurement methods. PACS measurement time: 18.53 ± 1.44 s; iPhone measurement time: 14.02 ± 1.08 s, iPhone demonstrating statistically significant faster measurement times than PACS, P < 0.05.
Conclusion
Using the iPhone’s built-in photo editing function to rapidly measure the parameters of the spinal- pelvic sagittal plane balance in the lumbosacral region is relatively accurate and reliable. This might provide a great convenience for Orthopedists in their clinical works, because they can measure imaging pictures with their iPhones at any time and place.
Keywords
iPhone
Lumbar lordosis
Pelvic tilt
Sacral slope
Fast measurement

1 Background
Spine-pelvic parameters refer to the measurable aspects of spine-pelvic sagittal balance. They are considered an important aspect of sagittal parameters, which include thoracic kyphosis (TK), lumbar lordosis (LL), pelvic Incidence (PI), pelvic tilt (PT) and sacral slope (SS), in which TK and LL are spinal parameters, and PI, PT and SS are pelvic parameters. The geometric relationship between the three parameters is PI = PT + SS1. The pelvis adjusts the trunk gravity center via rotation of the sagittal plane, which is axis-centered with the hip joint. This influences the physiological curvature of the lumbar vertebra, thoracic vertebra and cervical vertebra, to adjust the sagittal balance of the entire spine2. Imbalance in the sagittal spinal plane can lead to the development of an abnormal spine. The measurement of lumbosacral region spine-pelvic parameters is thus important in the evaluation of the spine’s entire sagittal balance. In this study, we used the built-in image processing application in the iPhone to rapidly measure LL, PT and SS parameters. We compared the measurements obtained on an iPhone with those obtained using PACS (Picture Archiving and Communication Systems), and evaluated the accuracy of both. Are there differences in accuracy and time-consuming between the two methods? Is the iPhone more convenient than PACS? We will make a discussion in this article. This study was approved by the medical ethics committee of Lanzhou University Second Hospital with the following reference number: 2017A-094. Data were only used for medical research and not for other purposes. The article includes pictures without patient names, and does not reveal patient information.
2 Methods
2.1 Patient selection
The study consisted of 28 female patients and 22 male patients aged 24–65 years (average age of 44 years), evaluated from January to September 2016. The inclusion criteria were as follows: normal lumbosacral vertebra and hip joint; no congenital or abnormal disease able to affect measurement; ability to participate in filming of the standard standing position of the whole spine by x-ray or three-dimensional CT of the lumbosacral region, which was required to clearly image the whole lumbar vertebra, sacrum and bilateral caput femoris.
2.2 Measurement of lumbosacral region spine-pelvic parameters with PACS
We first localized the sagittal plane in x-ray images or lumbosacral region three-dimensional CT scans to measure LL, PT and SS3. LL is the Cobb angle formed by the upper endplate connecting line of L1 and the upper endplate connection line of L2. PT is the included angle formed by the connecting line between the midpoint of the sacral endplate and the circular center of the caput femoris. If the bilateral caput femoris did not overlaps with the midpoint of the connecting line between the bilateral circular center. SS is the included angle formed by the connecting line between the sacral upper endplate and the level line. We used the built-in measurement tool in PACS to mark and measure every spinal-pelvic parameter angle (Fig. 1). This was conducted by two experienced doctors from the radiology department and the spinal surgery department. To reduce any measurement deviation induced by the observer, each angle was measured three times over 1 week, and the average of three measurements was taken to produce the final value.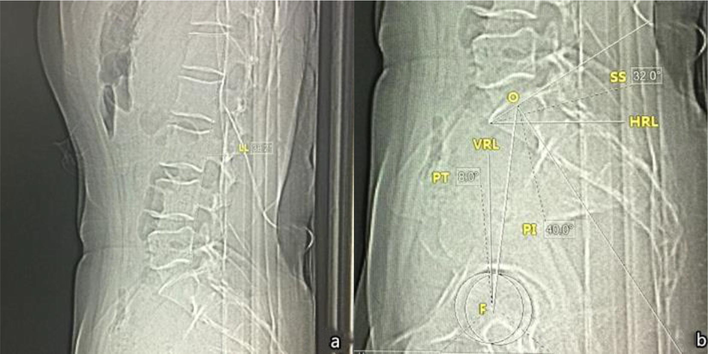
Measuring lumbosacral region spinal-pelvic parameters with PACS. a. LL = 38.2° b. O: Upper endplate midpoint of sacrum; F: Circular center of bilateral caput femoris; VRL: mid vertical line; HRL: horizontal line. SS = 32°PT = 8°; PI = SS + PT = 40°.
2.3 Measuring lumbosacral region spinal-pelvic parameters
One week after the measurements were performed using PACS, the same two investigators used the iPhone to measure LL, PT and SS. Investigators used the built-in camera of iPhone to take pictures without any marks (Fig. 2). During image acquisition, the camera lens was kept parallel with the imaging materials. Next, the iPhone’s built-in photo editing application was used to rotate the pictures, allowing the angle rotation scale and grid lines to clearly appear (Fig. 3). We determined that the prompt for rotating clockwise is positive, and negative for rotating counterclockwise, and that the smallest unit of rotation is 2° (Fig. 4).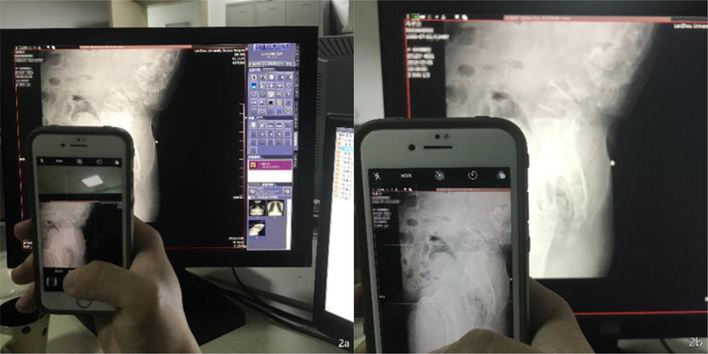
Use of the iPhone's speed dial mode to take pictures. a. Take pictures. b. Keep pictures at a level position.
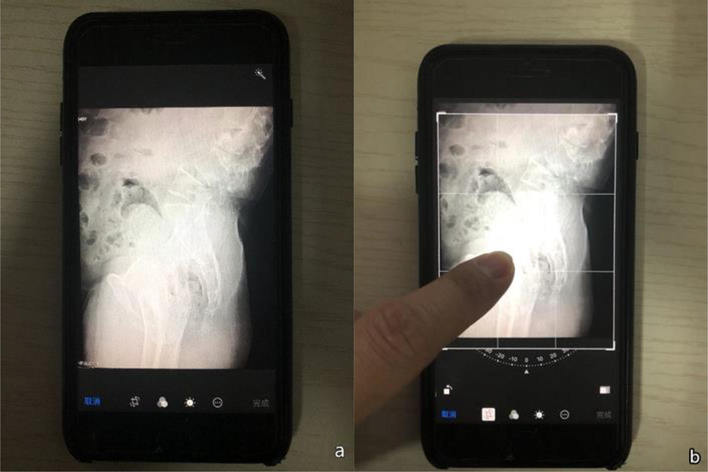
Choose the pictures to be edited. a. Select the target pictures. b. Click the Edit function, and choose the Picture Rotation and Crop function to rotate the target pictures.
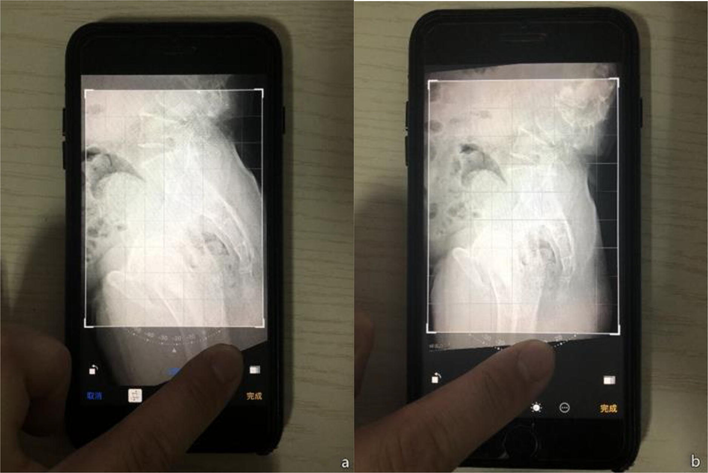
Rotate the pictures according to scale. a. Rotation of pictures clockwise. b. Rotation of pictures counter-clockwise.
According to the theory of end vertebra tilt angle (un-published research), pictures can be rotated until the visually-inspected connecting lines of the sacrum’s upper endplate overlap, or are parallel to, the horizontal grid lines; this rotated angle is SS. A rotation angle is formed when the visually inspected connecting line of the L1 vertebrae runs parallel with, or overlaps, the level grid lines; this angle plus SS is LL. Rotating the picture until the sacrum’s upper endplate and the visually-inspected midpoint of the caput femoris are parallel or completely overlap with the inter-vertical grid lines produces PT, which is the absolute value of the rotated angle (Fig. 5). Each measurement was taken three times per week, and the average value was obtained to produce the final parameter value.
Measuring lumbosacral region spinal-pelvic parameters with an iPhone. a. Visually inspect to confirm that the sacrum’s upper endplate connecting line overlaps with the level line, SS = 32°. b. Visually inspect to confirm that the endplate connecting line of L1 overlaps with the level line, and that the angle formed is 6°; LL = 38°. c. Visually inspect to confirm that the midpoint of the sacrum’s upper endplate connecting line and the central point of the bilateral caput femoris overlap on the same vertical line, PT = 8°.
2.4 Statistical processing
The statistical software SPSS 23.0 (IBM Corp. Armonk, NY, USA) for Mac was used to analyze data. Data are reported as the “mean ± standard deviation”. A Mann-Whitney U test was used to compare measurement results obtained using the iPhone vs. PACS. A one-way analysis of variance was used to analyze the differences between groups. A two-way random intra-class correlation coefficient was used to analyze the reliability of the two methods of measurement4. In cases where the measurement obtained by iPhone was greater than that of PACS, the parameter was defined as positive, and the inverse as negative. This was used to calculate measurement errors between the groups. The confidence interval for statistical analysis of the data was 95%. A P value < 0.05 was considered statistically significant.
3 Results
The parameter measurements obtained using PACS were as followings: LL average: 53.56 ± 15.76°; PT average: 12.60 ± 5.15°; SS average: 42.16 ± 13.29°. The parameter measurements obtained using the iPhone were as followings: LL average: 52.20 ± 14.46°; PT average: 12.48 ± 5.39°; SS average: 42.60 ± 12.33°. When compared, the measurements obtained using the two methods were not significantly different (iPhone LL vs. PACS LL: P = 0.707; iPhone PT vs. PACS PT: P = 0.961; iPhone SS vs. PACS SS: P = 0.702). Thus, both methods can be used to measure lumbosacral spine-pelvic sagittal balance parameters. The intra-class correlation coefficients (ICCs) of LL, PT, SS were 0.938, 0.812, and 0.946, thus the two measurement methods (iPhone vs. PACS) were highly correlated. The measurement deviations between iPhone and PACS were as follows: LL = (−7.33 ± 1.24°) (−20° to 19°); PT = (4.81 ± 0.68°) (−12° to 10°); SS = (5.87 ± 0.83°) (−9° to 17°). The deviation in measurement between the two groups was not statistically significant: (F = 0.202, P = 0.654; F = 0.112, P = 0.739; F = 0.029, P = 0.864; Figs. 6 and 7). The measurement time of the two methods (PACS vs. iPhone) was significantly different: PACS measurement time: 18.53 ± 1.44 s, iPhone measurement time: 14.02 ± 1.08 s, n = 15, P < 0.05; iPhone measurement time was faster than PACS measurement time by about 4.5 s (Fig. 8).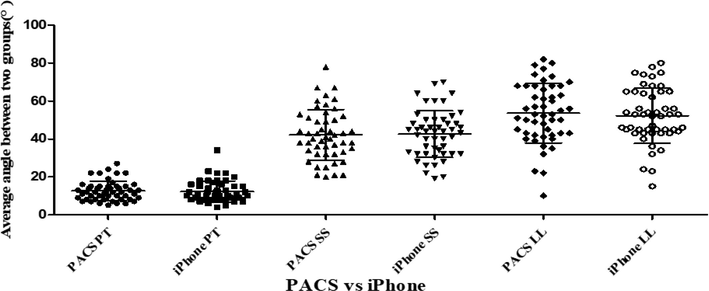
Lumbosacral region spinal-pelvic parameters using either rapid measurement by iPhone or PACS. n = 50, iPhone PT vs. PACS PT: P = 0.961; iPhone SS vs. PACS SS: P = 0.702; iPhone LL vs. PACS LL: P = 0.701. There was no significant difference between the two methods (P > 0.05).
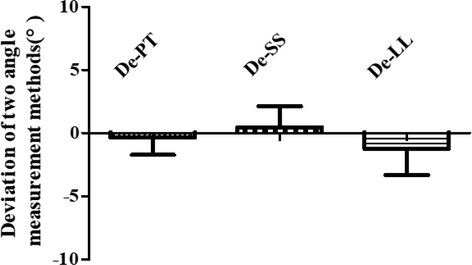
Lumbosacral region spinal-pelvic parameter deviation values between iPhone- and PACS-obtained measurements. The deviation in measurement between the two groups was not statistically significant (De-PT: F = 0.112, P = 0.739; De-SS: F = 0.029, P = 0.864; De-LL: F = 0.202, P = 0.654).
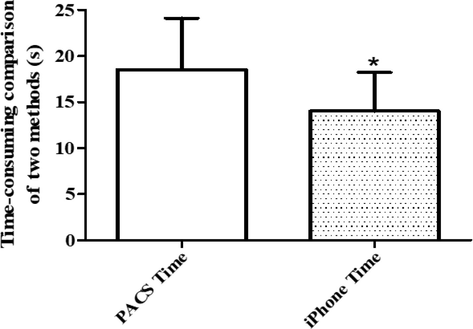
PACS measurement time vs iPhone measurement time. Data display the mean ± SD (n = 15, *P < 0.05, significantly different compared to the PACS group).
4 Discussion
Lumbosacral region spinal-pelvic sagittal plane balance parameters are closely related to the clinical lumbar degeneration and its development: When the spine is in degeneration, LL will gradually lose (Roussouly et al., 2005; Labelle et al., 2005). While the pelvis will keep the spinal sagittal plane in balance with compensatory back forward. PI and PT decrease (Labelle et al., 2005; Sebaaly et al., 2018; Schwab et al., 2012). SS takes part in forming of LL, and is related to lumbar lordosis, and also adjusts spinal-pelvic sagittal plane balance together with TK coupling (Bess et al., 2015; Schwab et al., 2010; Yamato et al., 2015).
Nowadays, many smartphones, such as iPhone, equipped with high-resolution screen and HD camera, and image processing editing software are also fully mature, which meaning that they may have impacts on the efficiency and convenience of rapid measurement of spinal pelvic sagittal balance parameters, that will provide a new technical approach for digital accurate angle measurement (Boulos et al., 2011; Franko, 2011; Kiser, 2011). Newer, simpler and more accessible smartphone’s APPs to measure Cobb angle, Acetabular prosthesis angle, end vertebra selection, early detection of spinal deformities and axial trunk rotation are emerging (Shaw et al., 2012; Wang et al., 2016; Pepe et al., 2017; Izatt et al., 2012; Driscoll et al., 2014; Franko et al., 2012; Sudarshan et al., 2016; Qiao et al., 2014; Qiao et al., 2012; Allam et al., 2016). In addition, researches have showed that when using cell phone sensors to measure clinical parameters, iPhone is more accurate than Android phones in orthopedics. Some applications have been invented for measuring Cobb angle of scoliosis, for example, Scoliometer (Izatt et al., 2012), Scolioscreen (Driscoll et al., 2014), scoligauge (Franko et al., 2012; Qiao et al., 2014); Tiltmeter (Shaw et al., 2012). The measurement principle of these Apps is to sense the angle change through the phone's built-in level sensor by rotating the mobile phone. Some apps like CobbMeter (Qiao et al., 2012; Allam et al., 2016) have similar measurement principles with PACS measurement method: The scoliosis imaging data was captured by the mobile phone camera, and the Cobb angle was automatically calculated by a program algorithm after marking the end vertebral endplate. This kind of dedicated software measurement method achieves good measurement accuracy and consistency between and within groups, relatively simple and easy to use, besides this method can save about 63% of time compared to manual methods (Sudarshan et al., 2016), even replace PACS to a certain extent (Prowse et al., 2016). However, using smartphone software to measurement also have drawbacks: firstly, this kind of software is often out of date and even never updated, this study has found that such software can not compatible with existing iPhone’s IOS system, Secondly, theoretically, there will always be certain bugs and errors in third-party software, and the stability is not as good as the software built in the system. Thirdly, some software is not free to use and requires additional costs.
In modern medical healthcare systems with digital radiographs and analyses, PACS and some else similar systems can measure in high accuracy, so that can be taken for standard of the parameter measurement. However, developing countries still analyses radiographs on conventional X-ray films, PACS systems are not popular in those areas because of expensive, so there is still a lot of angle measurement work that requires doctors to manually draw a line on the film with a protractor and a marker. In addition, in China, digitized information of imaging data is rarely stored on CD-ROM or USB Disc for clinicians and patients to communicate the condition, because most doctors' offices are not equipped with computer to retrieve and view these imaging information. We often face so many scenes in our country, When some patients come to a clinic with the imaging pictures which taken by other hospitals, the PACS system of the visiting hospital cannot match the imaging films of the previous hospitals, so the clinicians have to measure and analysis lumbosacral parameters through their eyes, protractor and pens.
Nearly everyone holds a smartphone, which is small in size and easy to carry. As a very convenient tool, smartphone can be totally used for measuring all parameter angles of spine after shooting image film directly to acquire the specific parameters in time, which is beneficial to judging the state of illness. Besides, smartphone has rich social functions. Many spine surgery doctors communicate on professional contents and upload the data and photos about the state of illness of many patients for remote consultation and discussion via social software such as group function of WeChat. By this way, the iconography data and photos of spine can be downloaded to phones and then alignment angle measurement of vertical plane of lumbosacral portion can be carried out via the photo editing program designed in iPhone.
We can shoot iconography data directly or download iconography photos via iPhone camera to measure the angle parameter of lumbosacral portion. The built-in Photo App of the system can be used stably and reliably with no software fault or extra fees. Only an iPhone is needed for software downloading.
According to the previous studies, the measurement results of spine malformation parameters acquired via iPhone have no obvious difference with the results obtained through other conventional methods (Shaw et al., 2012; Wang et al., 2016; Qiao et al., 2012; Hayes et al., 2013; Sudarshan et al., 2016). It has showed that the present spinal parameters measurement has many sources of errors (Capasso et al., 1992): an atypia position of patients in radiologic examination. To verify the accurate marker lines in the spinal segments which have anatomical variation of the vertebrae, different observers identify the different mark points/lines. This iPhone method is a digitized improvement, which has the similar measuring errors as the PACS method (Dickson et al., 1984). The efficacy and effectiveness of the iPhone method were observed and compared by the same observers via using the same medical images. Therefore, the very common errors are intrinsic to the measurement method. The iPhone method needs to make sure the reference points on the pictures, and it is difficult to make an accurate judgment about those points associated with the observers' eyes. And if the phone's camera is not perpendicular to the film when take a picture, the horizontal and vertical lines are not the same as the actual. It seems like to make measuring error, but it has confirmed that no obvious error in our previous study (Wang et al., 2018).
In this study, we studied the difference of results of angle parameter iconography and radiology angle of vertical plane of human body spine and pelvis by using iPhone technology and PACS technology. As with similar previous studies (Franko et al., 2012), the parameters of sagittal view of all lumbosacral portion acquired by phone are highly consistent with the results measured by PACS. The difference between the results measured by iPhone and PACS is very small and the average error is 5°–7°, bias 0.68°–1.24°. Therefore, it can be concluded that iPhone is a kind of method for spine parameters with high precision.
In addition, this research group appears that in two ways of measuring PT, LL and SS, the ICC of PT is less than that of LL and SS (0.812 VS 0.938 VS 0.946). It is considered that fast visual measurement of SS, LL and PT needs to ensure two marked dots on sacral upper endplate connection line, and ensure the four measurement mark points upper on lower vertebral and plate connection lines, and ensure the endplate connection midpoint on sacrum and the midpoint and central point of bilateral femoral heads. In the measurement process, increasing interference factors would lead to low consistence. If measurement marks are pre-marked, the potential reliability of two measurement results are better. While that, to some extent, decrease the convenience for using smart phones to directly shoot image of image materials to fast read the parameters.
This research is about using the iPhone’s built-in photo program to measure the parameters of lumbosacral region spinal-pelvic sagittal position. On the basis of the measurement accuracy, it is more convenient and faster to using the iPhone for measurement than the traditional measurement by hand-drawn lines, and having similar accuracy with PACS. This is an absolutely new way for improving clinical work efficiency. Due to the limited space, this research is not yet involved with how to use the iPhone to measure the feasibility of TK (the Cobb angle of upper endplate of T4 and lower endplate of T12), thoracic inlet angle, T1 slope, neck tilt and some other spinal-pelvic sagittal plane balance parameters (Lee et al., 2012). But according to the same geometry definition on the similar parameters, this iPhone measurement method could be still accurate and reliable with the similar kind of clinical parameters.
5 Conclusions
This study assessed the ability of the iPhone’s built-in photo application to measure the parameters of lumbosacral region spinal-pelvic sagittal balance. It is more convenient and faster to use an iPhone for measurement vs. a traditional manual analysis, and it shows similar measurement accuracy when compared with PACS. Given our present findings demonstrating the acquisition of similar spinal parameters, iPhone-aided measurement is likely to be an accurate and reliable method for many other clinical parameters.
Declaration of Competing Interest
All authors declare that there are no competing interests in this article.
Acknowledgments
This study was conducted at Orthopedics Key Laboratory of Gansu.
Province, Orthopedics Department and Radiology Department of Lanzhou University Second Hospital, Lanzhou University, Lanzhou, China.
Ethics approval and consent to participate
This study was approved by the medical ethics committee of Lanzhou.
University Second Hospital with the following reference number: 2017A-094. Data were only used for medical research and not for other purposes.
Funding
There is no any funding for this research.
References
- Comparison between Oxford Cobbmeter and digital Cobbmeter for measurement of Cobb angle in adolescent idiopathic scoliosis. Eur. Spine J.. 2016;25(2):444-449.
- [Google Scholar]
- Clinical and radiographic evaluation of adult spinal deformity. J. Spinal Disord. Tech.. 2015;2(29):6-19.
- [Google Scholar]
- How smartphones are changing the face of mobile and participatory healthcare: an overview, with example from eCAALYX. Biomed. Eng. Online. 2011;10:24.
- [Google Scholar]
- The validity and reliability of measurements in spinal deformities: a critical appraisal. Acta Orthop. Belg.. 1992;58(2):126-135.
- [Google Scholar]
- The pathogenesis of idiopathic scoliosis. Biplanar spinal asymmetry. J. Bone Joint Surg. Br.. 1984;66(1):8-15.
- [Google Scholar]
- Evaluation of an apparatus to be combined with a smartphone for the early detection of spinal deformities. Scoliosis. 2014;9(1):10.
- [Google Scholar]
- Smartphone apps for orthopaedic surgeons. Clin. Orthop. Relat. Res.. 2011;469:2042-2048.
- [Google Scholar]
- Validation of a scoliometer smartphone app to assess scoliosis. J. Pediatric Orthop.. 2012;32(8):e72-e75.
- [Google Scholar]
- Validation of a scoliometer smartphone app to assess scoliosis. J. Pedia Ortho. 2012;32(8):72-75.
- [Google Scholar]
- A systematic review of all smart phone applications specifically aimed for use as a scoliosis screening tool. Spine. 2013;13(9) S38–S38
- [Google Scholar]
- Evaluation of the iPhone with an acrylic sleeve versus the Scoliometer for rib hump measurement in scoliosis. Scoliosis. 2012;7(1):1-8.
- [Google Scholar]
- 25 ways to use your smartphone. Physicians share their favorite uses and apps. Minn. Med.. 2011;94:22-29.
- [Google Scholar]
- The importance of spinopelvic balance in L5–s1 developmental spondylolisthesis: a review of pertinent radiologic measurements. Spine. 2005;30(6 Suppl):S27.
- [Google Scholar]
- The influence of thoracic inlet alignment on the craniocervical sagittal balance in asymptomatic adult. Spinal Disord. Tech.. 2012;25(2):41-47.
- [Google Scholar]
- Use of the smartphone for end vertebra selection in scoliosis. Acta Orthop. Traumatol. Turc.. 2017;51(2):146-149.
- [Google Scholar]
- Reliability and validity of inexpensive and easily administered anthropometric clinical evaluation methods of postural asymmetry measurement in adolescent idiopathic scoliosis: a systematic review. Eur. Spine J.. 2016;25(2):450-466.
- [Google Scholar]
- Reliability analysis of a smartphone-aided measurement method for the Cobb angle of scoliosis. J. Spinal Disord. Tech.. 2012;25(4):E88.
- [Google Scholar]
- Inter- and intraobserver reliability assessment of the axial trunk rotation: manual versus smartphone-aided measurement tools. BMC Musculoskeletal Disord.. 2014;15(1):343.
- [Google Scholar]
- Classification of the normal variation in the sagittal alignment of the human lumbar spine and pelvis in the standing position. Spine. 2005;30(13):1558.
- [Google Scholar]
- Adult spinal deformity-postoperative standing imbalance: how much can you tolerate? An overview of key parameters in assessing alignment and planning corrective surgery. Spine. 2010;35(25):2224-2231.
- [Google Scholar]
- Scoliosis Research Society-Schwab adult spinal deformity classification: a validation study. Spine. 2012;37(12):1077-1082.
- [Google Scholar]
- Description of the sagittal alignment of the degenerative human spine. Eur. Spine J.. 2018;27(2):489-496.
- [Google Scholar]
- Use of the iPhone for Cobb angle measurement in scoliosis. Euro Spine J.. 2012;21(6):1062-1068.
- [Google Scholar]
- Measuring Cobb's angle in scoliosis: can smartphones match manual methods and software based analysis? A three way crossover study. Glob. Spine J.. 2016;06(S 01)
- [Google Scholar]
- Use of smartphone in acetabular component angle measurement during total hip arthroplasty. Chin. J. Repair. Recons. Surg.. 2016;30(9):1061-1064.
- [Google Scholar]
- Measurement of scoliosis Cobb angle by end vertebra tilt angle method. J. Orthop. Surg. Res.. 2018;13(1):223-270.
- [Google Scholar]
- Calculation of the target lumbar lordosis angle for restoring an optimal pelvic tilt in elderly patients with adult spinal deformity. Spine. 2015;41(4)
- [Google Scholar]




