

Translate this page into:
Forensic significance of cTnI serum for the detection of terminal myocardial damage in rats (Rattus norvegicus) caused by hyperthermia
⁎Corresponding author. zurifa.ajanovic@mf.unsa.ba (Zurifa Ajanović)
-
Received: ,
Accepted: ,
This article was originally published by Elsevier and was migrated to Scientific Scholar after the change of Publisher.
Peer review under responsibility of King Saud University.
Abstract
Figure 2. Difference in values of repeated measurement of cardiac troponin I in rat serum in experimental groups. The values of the cardiac isoform of troponin I are presented in the form of a median with an interquartile range (25–75 percentile). Vertical lines represent the range of minimum and maximum values. cTnI- cardiac isoform of troponin I (b-basal values; p-repeated measurements); p-probability; KG37-control group of rats exposed to water temperature of 37 °C; G41 group exposed to water temperature 41 °C.

Abstract
Objectives
To determine whether the biochemical marker cTnI with circulating value has forensic significance in the detection of myocardial damage in rats in experimental conditions of hyperthermia by exposure to water temperatures of 41 °C.
Material and methods
The study was conducted on 24 adult Wistar rats that were divided into two experimental groups, depending on water temperature exposure of 37 °C (KG, n = 8) and 41 °C (G41, n = 16). Depending on the length of time of exposure to water temperatures of 41 °C are further divided into G41-AM (20 min of exposure), G41-PM (exposure until death). Blood for analysis of the concentration of cardiac troponin I (cTnI) was taken before the experiment and after the expiration of the given duration of the experiment of 20 min or death. The concentration of cTnI was determined in serum by ELISA method. The level of statistical significance was, p < 0.05.
Results
Eight rats of the G41 group achieved a core temperature that is the threshold for heat stroke. The median survival time for group G41 was 175.5 min. The median cTnI was 358.64 for group KG 37. The control group of rats had significantly lower serum cTnI values compared to G41. Examination of the length of exposure to appropriate temperatures led to significant increases in cTnI in the serum; A significant difference was found in the values of cTnI KG37 and G41-PM. CTnI values differed significantly in the G41-AM and G41-PM groups. In G 41 °C, a positive correlation was found between serum cTnI values and body temperature measured in fatal outcome.
Conclusions
CTnI with their changes in serum concentration indicate exposure to high water temperature.
Keywords
Hyperthermia
Cardiac protein I
Myocardium
Forensic significance

1 Introduction
There are more and more deaths in the world that occur indoors with an increase in indoor air temperature, for example in the bathroom, during bathing, or in Turkish baths or saunas. Autopsy rates are generally low and vary widely across countries with rates below 10% of all deaths within the U.S., compared to 23.8% in Finland, and autopsy protocols in cases of suspected sudden cardiac death also vary, even within region of countries. These differences in autopsy rates and protocols are likely to contribute to differences in the incidence and causes of sudden cardiac death (Hayashi et al, 2015). Scientific data on the role and association of hyperthermia as a cause of sudden cardiac death are scarce and further research is needed in this field. Current science suggests that hyperthermia and the cardiac response are causally related according to the very pathophysiological sequence of events in hyperthermia. In the forensic sense, there is scarce evidence of a pathophysiological mechanism leading to sudden cardiac death. (Myerburg and Junttila, 2012) (Table 1). n-number of rats; KG37-control group of rats exposed to water temperature of 37 °C; G41-group exposed to water temperature of 41 °C.
Variable
Groups
KG37
G41
Heat stroke (n,%)
No
N
7
7
% in group
100.0%
46.7%
%of total number
18.4%
18.4%
Yes
N
0
8
% in group
0.0%
53.3%
% of total number
0.0%
21.1%
In the field of forensic medicine, a biochemically adequate marker was sought that would be the gold standard for cardiomyocyte damage postmortem to detect the mechanisms that cause terminal cardiomyocyte damage. Cardiac troponin I (cTnI) is characteristic of cardiac muscle fibers. According to the research of Hasić et al (2007), minimal circulating values of cTnI were determined, but no significant gender differences were observed in healthy subjects. Its increase in circulation is specific for myocardial damage, but does not indicate the mechanism of the resulting damage (Al-Otaiby et al, 2011).
In recent years, heat stroke has very rarely been reported as a possible cause of elevated cTnI, although heat stroke has been associated with an increased risk of sudden cardiac death (Hausfater et al., 2010a; Hausfater et al., 2010b; Pease et al, 2009). In a study by Hausfater et al. (2010a), Hausfater et al. (2010b) observed elevated cTnI was often associated with elevated ambient temperature (52%). Nineteen percent of these patients had a severe increase in cTnI suggesting severe myocardial damage. At temperatures above 40 °C, elevated cTnI was associated with death. Elevated cTnI may occur in the absence of acute coronary syndrome during heat stroke (Zhu et al, 2007).
The aim of this study was to determine whether the biochemical marker cTnI with circulating value has forensic significance in the detection of myocardial damage in rats in experimental conditions of hyperthermia by exposure to water temperatures of 41 °C.
2 Material and methods
The study was conducted as a prospective, randomized, controlled, experimental study on animal sample of rats (Rattus norvegicus) on which hyperthermia was induced. The study was conducted at Medical Faculty and at Veterinary Faculty University of Sarajevo, in accordance with the applicable ethical principles on biomedical research on animals (the Council for International Organizations of Medical Sciences) and ICLAS (The International Council for Laboratory Animal Science), approved by the Ethics Committee Faculty of Medicine (02–3-4–1253/20) as well as the consent of the Department of Pathological Physiology of the Faculty of Veterinary Medicine, University of Sarajevo (No. 02–3/720/19).
The study was conducted on 24 adult Wistar rats that were methodologically divided into two experimental groups, depending on water temperature exposure of 37 °C (KG, n = 8) and 41 °C (G41, n = 16). Depending on the length of time of exposure to water temperatures of 41 °C are further divided into G41-AM (20 min of exposure), G41-PM (exposure until death).
The age of the examined rats was between 3.5 months and 4 months, weight of the rats was between 250 g and 310 g, and 14 rats were male and 8 rats were female.
Wistar rats were kept in a vivarium with a 12-hour light regime day-night at the room temperature 7 days before the experiment for acclimatization and adaptation. During the experiment, the animals received commercial feed for laboratory animals and running water ad libitum.
In this study, the thermoregulatory response of the rat organism was monitored by exposing the rats to a water temperature of 37 °C-KG37 and 41 °C-G41. A change in core temperature was recorded using an esophageal catheter placed in anesthetized rats. According to the literature, the physiological body temperature of rats was 37.5–37.7 °C , and the aim was to develop a model of hyperthermia and record the frequency of core temperature ≥ 40.05 °C which is the temperature threshold for heat stroke (Delibegovic et al., 2016).
2.1 Induction of hyperthermia on a rats model
We filled the water bath with water and heated it to the target water temperature. The water temperature was continuously monitored on the display with additional measurement with a probe immersed in water and reading on a thermometer. We immersed a previously anesthetized rat with the head above the water level, fixed on a wooden board, in preheated water of the target temperature. Survival time was recorded, which included the time from immersion of rats in water of a given temperature (41 °C) to the time of death. We defined hyperthermia as an increase in internal temperature by 0.5 °C, and heat stroke as an increase in internal temperature above 40.5 °C (Kidane and Peters, 2020).
2.2 Sampling
Blood for analysis of the concentration of cardiac troponin I (cTnI) was taken before the experiment and after the expiration of the given duration of the experiment of 20 min or death. The concentration of cTnI was determined in serum by ELISA method. The level of statistical significance was p < 0.05.
Cardiac TnI concentration was determined in serum by an enzyme-linked immunosorbent enzyme-linked enzyme (Enzyme Linked Immuno Sorbent Assay ELISA reader, type 2100, Statfax, USA). The cardiac isoform of troponin I was determined in rat serum by sandwich ELISA. A microtiter plate coated with rat cTnI-specific antibodies was used. Upon addition of the standard and sample, the antigen–antibody reaction takes place on the wall of the microtiter well and complexes are formed. In the next step, biotinylated rat cTnI-specific detection antibody and horseradish avidin peroxidase conjugate are successively added and incubated. Unbound material is washed. Substrate solution was further added, and wells containing rat cTnI, biotinylated detection antibody, and horseradish avidin peroxidase conjugate were both blue. The enzyme-substrate reaction is stopped by the addition of a stop solution and the colour changes to yellow. Optical density is measured spectrophotometrically at a wavelength of 450 ± 2 nm. The value of the optical density is proportional to the concentration of cTnI in rats. Sample: serum; Sensitivity 18.75 pg/ml; Detection range 31.25–2000 ng /ml.
3 Results
Frequency analysis of rats with a body temperature of 40.05 ◦C and higher, showed that it was highest in a group G41 of eight rats (Table 1).
The Kaplan Mayer curve analyzed the rats survival time exposed to water temperatures of 41 °C (G41-PM). Survival was higher in the group exposed to lower water temperature because the mean value in G41 was 175.50 min (Table 2). G41-PM- postmortem group rats exposed water temperature of 41 °C (length of exposure to death).
Median survival time (minuts)
Groups
Mean
Median
SE
95% IP
Xmed
SE
95% IP
DG
GG
DG
GG
G41-PM
175.50
31.03
114.66
236.33
168.00
11.31
145.82
190.17
The Kruskal-Wallis H test showed that the mean values of basal serum cTnI concentrations before exposure to the appropriate water temperature differed significantly p = 0.023, with mean rank values for groups being 12.43 pg/ml in KG37, 16.40 pg/ml in G41 (Table 3). The values of cTnI (pg/ml) are represented by the median along the interquartile range (25–75 percentile), cTnI-b-basal values of the cardiac isoform of troponin I; KG37-control group of rats exposed to water temperature of 37 °C; G41 group exposed to water temperature 41 °C.
Variable
Group
X25
Xmed
X75
cTnI-b (pg/ml)
KG37
56.32
81.17
190.86
G41
72.64
119.37
258.00
The control group of rats had significantly lower cTnI values compared to G41 (p = 0.023).
The control group of rats had significantly lower cTnI values compared to G41 (p = 0.023) (Fig. 1).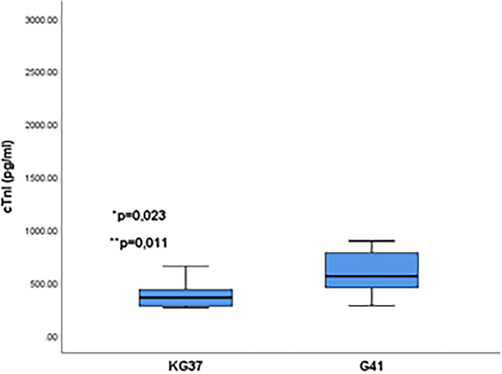
Significance of the difference in the serum concentration of cardiac troponin I in the control group in relation to the G41 group. The values of the cardiac isoform of troponin I are presented in the form of a median with an interquartile range (25–75 percentile). Vertical lines represent the range of minimum and maximum values. cTnI-cardiac isoform of troponin I; p-probability; KG37-control group of rats exposed to water temperatures of 37 °C; G41 group exposed to water temperature 41 °C; ⁎ represents the relationship of significance between KG37 and G41.
Fig. 2 shows the differences and the significance of the difference in cTnI concentrations before and after exposure to water temperature depending on the experimental group. The smallest difference in the repeated measurement was induced by the water temperature of 37 °C (p = 0.028). In the G41 groups (p = 0.001), serum cTnI concentrations increased relative to the basal value, which showed statistically significant difference of the cTnI concentration in both groups, p = 0.001 (Fig. 2 and Table 4). CTnI values (pg/ml) are represented by the median along the interquartile range (25–75 percentile), cTnI-p-repeated measurement of cardiac isoform troponin I; KG37-control group of rats exposed to water temperature of 37 °C; G41 group exposed to water temperature 41 °C.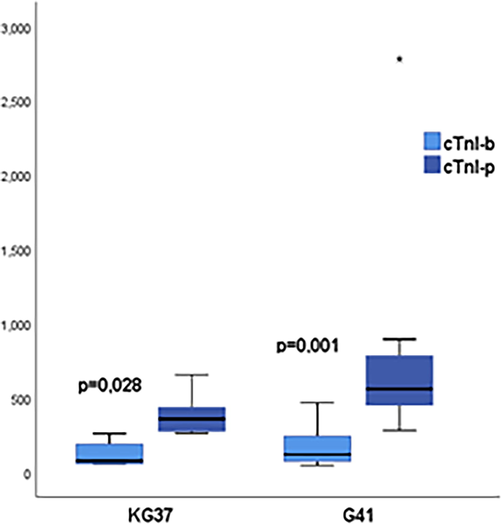
Difference in values of repeated measurement of cardiac troponin I in rat serum in experimental groups. The values of the cardiac isoform of troponin I are presented in the form of a median with an interquartile range (25–75 percentile). Vertical lines represent the range of minimum and maximum values. cTnI- cardiac isoform of troponin I (b-basal values; p-repeated measurements); p-probability; KG37-control group of rats exposed to water temperature of 37 °C; G41 group exposed to water temperature 41 °C.
Variable
Group
X25
Xmed
X75
cTnI-p (pg/ml)
KG37
273.41
358.64
490.34
G41
431.78
560.31
838.36
There was a statistically significant difference between the values of cTnI of the control group of rats and the group G41-PM (p = 0.005). The values of cTnI in the groups G41-AM and G41-PM differed significantly, p = 0.009 (Fig. 3).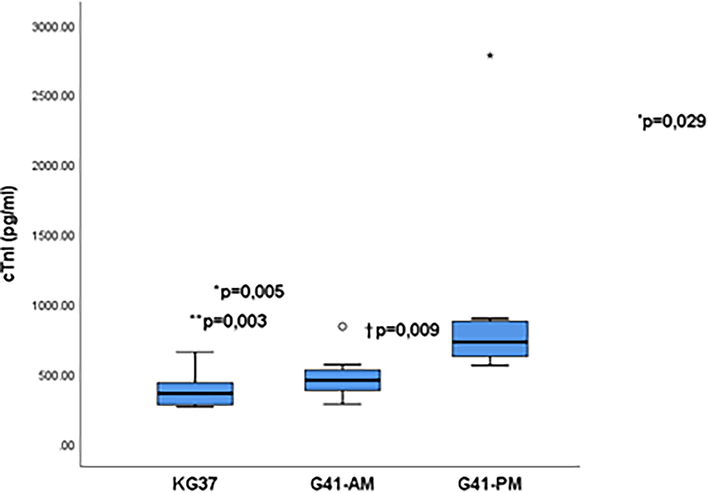
Influence of the length of exposure time of rats of experimental groups on differences in serum concentrations of cardiac troponin I. The values of the cardiac isoform of troponin I are presented in the form of a median with an interquartile range (25–75 percentile). Vertical lines represent the range of minimum and maximum values .; cTnI- cardiac isoform of troponin I; p-probability; * p KGvsG41-PM; † p G41AM vs G1-PM; KG37-control group of rats exposed to water temperatures of 37˚G41-AM- antemortem group exposed to water temperatures of 41 °C (length of exposure 20 min); G41-PM- postmortem group exposed to water temperature 41 °C (length of exposure to death); star and circle-extreme value of cTnI in the group.
Serum cTnI values ≥ 625.45 pg/ml can detect rats with terminal myocardial damage at temperature exposure of 41 °C, p = 0.011 (Fig. 4 and Table 5). AUC- area under the curve; PPV-positive predictive value, NPV-negative predictive value, 95% IP confidence interval; p-probability; cTnI-cardiac troponin I isoform.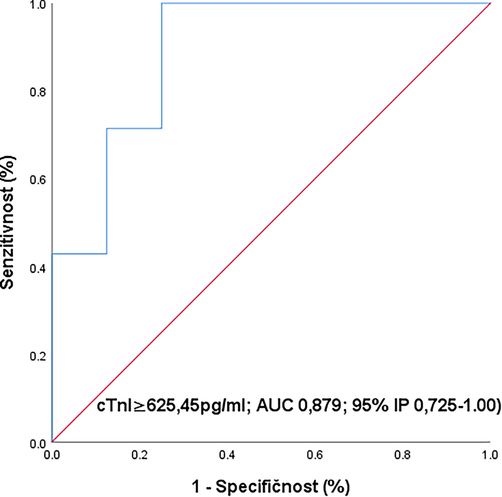
ROC curve of concentration cardiac troponin in serum as a biomarker of terminal myocardial damage in rats exposed to temperatures of 41 °C. ROC-Reciever Operating Characteristics; AUC-engl. Area under curve, IP-(CI-confidence interval); p-probability; cTnI-cardiac isoform of troponin I.
Varible
AUC
Sensitivity (%)
Specificity (%)
PPV (%)
NPV (%)
95% IP
p
cTnI (pg/ml)
0.893
71.0
87.5%
83.3
77.7
0.771–0.987
0.011
4 Discussion
Heat stroke is a condition of the body in which the body's compensatory mechanisms of internal temperature control weaken. As a fatal condition, heat stroke is characterized by an elevated core temperature of 40.05 °C and above, secondarily due to prolonged exposure to high ambient temperature (Suzuki and Hori, 2014). The condition can cause nervous system dysfunction, myocardial infarction, renal failure, and muscle dysfunction and is defined as a multisystem disorder of the body (Nzvere et al, 2020). A condition that leads to death in 10–50% of cases, and the cardiovascular abnormalities that accompany it are hypotension, electrolyte disturbance, malignant arrhythmia, ischemia, depression of heart function with global hypokinesia (Rajan et al, 2017). Understanding the physiological and behavioral response of animals, including humans, to elevated ambient temperature has gained in critical importance with global warming and with the expectation of an increase in the number and severity of heat waves (Barney and Kuhrt, 2016).
Identification of hyperthermia as a cause of death is usually difficult in forensic medicine due to nonspecific, incorrect, and even negative macroscopic and microscopic findings. In order to better understand the pathophysiology of fatal hyperthermia, numerous postmortem biochemical analyzes have been performed such as the concentration of electrolytes, hormones, blood proteins, enzymes, neurotransmitters in the blood or other biological fluids. Practical application requires it to be confirmed by studies in larger groups of deaths caused by hypertemia (Lin et al, 2019).
Autopsy findings become difficult if the body has been in a high temperature environment for a long time and very quickly enters the phase of the putrefaction process. Thus, for the diagnosis of death caused by hyperthermia, investigative actions and circumstances of death are extremely important. A significant difficulty faced by autopsies is the lack of unique diagnostic criteria for the diagnosis of heat-related death (Nixdorf-Miller et al, 2006).
In our study, we used the fact that troponin I is the gold standard that has a higher sensitivity and specificity for detecting myocardial cell damage compared to the catalytic activity of enzymes.
By examining the effect of temperature on cTnI values in the blood, we obtained significantly higher values in groups G41 (p = 0.023) compared to group KG37. The individual response to exposure to higher than body temperature was assessed by repeated measurements and comparison with basal values. All groups had significantly higher cTnI in the blood where for the control group-KG 37, p = 0.028, G41-p = 0.001, which implies significantly higher effects of water temperature of 41 °C on the release of cTnI from rat myocardium. Examination of the effect of exposure length showed that cTnI was significantly higher in the serum of rats with fatal outcome due to terminal hyperthermic damage compared to rats that were exposed for only 20 min and sacrificed. The survival time of group 41 was longer (mean 175 min). According to a study by Quinn et al. (2014). It is recommended to use cTnI as a sensitive marker in conditions of hyperthermia and heat stroke especially for the purpose of improving the treatment of myocardial damage during recovery from heat stroke.
Examination of the significance of cTnI as a biomarker of terminal myocardial damage at a water temperature of 41 °C showed that at a damage level of p < 0.05 serum cTnI concentrations ≥ 625.45 pg/ml (sensitivity 71.0%, specificity 87.5%, PPV 83.3%, NPV 77.7%; p = 0.011) indicates terminal cardiomyocyte damage at 41 °C exposure and may be a marker of terminal hyperthermic myocardial damage.
In the study conducted during 2003 in France, authors also analyzed cardiac troponin I (cTnI) concentration in patients during a 2003 heat wave in France. The authors concluded that cTnI is often elevated in patients with nonexertional heat-related illnesses during the heat wave and was an independent risk factor only in high-risk patients in whom increase of cTnI concentration (>1.5 ng.mL-1) indicated severe myocardial infarction (Hausfater et al., 2010a; Hausfater et al., 2010b).
Results of study from Audet et al. (2015) showed that the ctPOC test had high sensitivity and specificity in detecting heat stroke severity early in the heat stroke syndrome, while predicting multiorgan damage within 24 h of recovery.
Palmiere and Mangin (2013) in their research presented review of medical-legal literature related to postmortem biochemical tests associated with heat-related deaths including tests of cardiac markers.
Results of the study from Ying-Ming et al. (2002) showed that certain isoenzymes that is incorporated into myofibrils from the hearts are more sensitive to elevated temperature, and it can be expected that individuals with these isoenzymes will experience heat stroke earlier when exposed to temperature.
5 Conclusion
CTnI with their changes in serum concentration indicate exposure to high water temperature. From the forensic aspect, the significance of cTnI in serum for the detection of terminal myocardial damage was determined on a model of rat hyperthermia. This finding requires further validation on human material in order for cTnI to be included as a biochemical marker of terminal myocardial damage caused by hyperthermia.
This research did not receive any specific grant from funding agencies in the public, commercial, or not-for-profit sectors.
Conflict of interest
The authors confirm that there are no known conflicts of interest associated with this publication and there has been no significant financial support for this work that could have influenced its outcome. The study was conducted at Medical Faculty and at Veterinary Faculty University of Sarajevo, in accordance with the applicable ethical principles on biomedical research on animals (the Council for International Organizations of Medical Sciences) and ICLAS (The International Council for Laboratory Animal Science), approved by the Ethics Committee Faculty of Medicine (02–3-4–1253/20) as well as the consent of the Department of Pathological Physiology of the Faculty of Veterinary Medicine, University of Sarajevo (No. 02–3/720/19).
Declaration of Competing Interest
The authors declare that they have no known competing financial interests or personal relationships that could have appeared to influence the work reported in this paper.
References
- The clinical significance of cardiac troponins in medical practice. J. Saudi Heart Assoc.. 2011;23(1):3-11.
- [Google Scholar]
- Point-of-care cardiac troponin test accurately predicts heat stroke severity in rats. Am. J. Physiol. Regul. Integr. Comp. Physiol.. 2015;309(10):R1264-R1272.
- [Google Scholar]
- Formation of adhesion after intraperitoneal application of TiMesh: experimental study on a rodent model. Acta Chir. Belg.. 2016;116(5):293-300.
- [Google Scholar]
- Myoglobin et cardiac troponin I-biochemical markers of acute myocardial infarction. HealthMED.. 2007;1(3):94-99.
- [Google Scholar]
- Elevation of cardiac troponin I during non-exertional heat-related illnesses in the context of a heatwave. Crit. Care. 2010;14(3):R99.
- [CrossRef] [Google Scholar]
- The spectrum of epidemiology underlying sudden cardiac death. Circ Res.. 2015;116(12):1887-1906.
- [Google Scholar]
- Biochemical detection of fatal hypothermia and hyperthermia in affected rat hypothalamus tissues by Fourier transform infrared spectroscopy. Biosci. Rep.. 2019;39(3)
- [CrossRef] [Google Scholar]
- Sudden cardiac death caused by coronary heart disease. Circulation.. 2012;125(8):1043-1052.
- [Google Scholar]
- Hypothermia and Hyperthermia medicolegal investigation of morbidity and mortality from exposure to environmental temperature extremes. Arch. Pathol. Lab Med.. 2006;130(9):1297-1304.
- [Google Scholar]
- Long-term cardiovascular diseases of heatstroke: A delayed pathophysiology outcome. Cureus.. 2020;12(8):e95951
- [Google Scholar]
- Hyperthermia and postmortem biochemical investigations. Int. J. Legal Med.. 2013;127(1):93-102.
- [Google Scholar]
- Early organ dysfunction course, cooling time and outcome in classic heatstroke. ICM.. 2009;35(8):1454-1458.
- [Google Scholar]
- Cardiovascular and thermoregulatory biomarkers of heat stroke severity in a conscious rat model. J. Appl. Physiol.. 2014;117(9):971-978.
- [Google Scholar]
- Heat stroke manifesting as cardiac arrest and multi-organ failure. JCR. 2017;7:264-266.
- [Google Scholar]
- Experimental investigation in rats to identify the cause of sudden death during bathing in Japan. AMS.. 2014;1(2):101-104.
- [Google Scholar]
- Changes in thiol reactivity and extractability of myofibril bound cardiac troponin C in porcine malignant hyperthermia. J. Biochem.. 2002;132:317-325.
- [Google Scholar]
- Postmortem cardiac troponin I and creatine kinase MB levels in the blood and pericardial fluid as markers of myocardial damage in medicolegal autopsy. Leg Med.. 2007;9(5):241-250.
- [Google Scholar]




