

Translate this page into:
Effect of evidence-based care in continuous renal replacement therapy for severe pancreatitis and the effect on serum PCT, CRP levels, and CYP2C19 genotyping
⁎Corresponding author at: Department of Critical Medicine, Shijiazhuang 050051, Hebei, China. chunxialiu202204@163.com (Chunxia Liu)
-
Received: ,
Accepted: ,
This article was originally published by Elsevier and was migrated to Scientific Scholar after the change of Publisher.
Peer review under responsibility of King Saud University.
Abstract
This paper presents an in-depth study and analysis of evidence-based care in continuous renal replacement therapy for severe pancreatitis and examines the effects of serum procalcitonin (PCT), C-reactive protein (CRP) levels, and CYP2C19 genotyping. Eighty patients with severe pancreatitis who met the inclusion criteria were randomly assigned to the medium metabolic group and the slow metabolic group according to their CYP2C19 gene test results, and then the two groups were randomly divided into the control group and the observation group according to the different treatment regimens. Group 1 was CYP2C19 gene intermediate metabolism and was given to the control group; group 2 was CYP2C19 gene intermediate metabolism and was given to the observation group; group 3 was CYP2C19 gene slow metabolism and was given to the control group; group 4 was CYP2C19 gene slow metabolism and was given to the observation group. The number of cases in each group was 20, and follow-up was taken, but enteral nutrition also has some complications, such as feeding intolerance, if clinicians and nursing staff actively give effective care, it can significantly reduce the incidence of complications, and improve the value of enteral nutrition, shorten the hospitalization time, and improve the clinical prognosis. The relationship between serum CRP and PCT levels and Spatially Oriented Format for Acoustics (SOFA) score and the type of Virtual Access Point (VAP) pathogens and prognosis was investigated by Spearman correlation analysis. Finally, Pearson correlation analysis was used to investigate the relationship between serum CRP and PCT levels and SOFA scores in VAP patients. Based on the above analysis, the clinical value of CRP, PCT levels, and SOFA scores in VAP was evaluated. Several evidence-based guidelines were developed to provide clear recommendations and guidance for the preventive management of enteral nutrition feeding intolerance, but there is a gap between clinical care practice and the best evidence, so the best evidence was introduced. We compare the analysis of the test results with previously reported similar tests, and our results show good accuracy and higher efficiency.
Keywords
Evidence-based care
Severe pancreatitis
Renal replacement therapy
Effectiveness of application
Serum PCT and CRP levels
CYP2C19 genotyping

1 Introduction
Acute pancreatitis begins with increased pancreatic enzyme activity due to various etiologies, followed by a local inflammatory response in pancreatic tissue. Patients with severe acute pancreatitis will have a systemic inflammatory response syndrome and, in some cases, diseases such as multi-organ dysfunction syndrome. Acute pancreatitis mainly attacks the patient's digestive system, and the mechanism of this disease is complex, which not only poses a great threat to the patient's body but also brings more challenges to doctors in terms of clinical treatment. In recent years, the incidence of acute pancreatitis has been on the rise, and in clinical treatment, many patients with acute pancreatitis have a self-limiting course, with about 20 %–30 % of patients showing a high risk of acute pancreatitis at the time of treatment, and the lethality of acute pancreatitis reaching 5 %–10 %. Currently, the treatment of acute pancreatitis has gradually developed a model of multidisciplinary participation and the development of individualized programs (Pereira et al., 2021). However, we should not only be satisfied with the basic needs of treating the disease, but also use advances in medical technology to analyze, through a large number of studies, the pathogenesis of acute pancreatitis and the progression of the disease, so that clinical medical personnel can do the relevant clinical diagnosis and treatment measures to reduce the pain brought by the disease to patients, promote a harmonious doctor-patient relationship between doctors and patients, and accelerate the rapid recovery of patients. Severe acute pancreatitis is the most serious type of acute pancreatitis, and SAP occurs in about 15 %–25 % of patients with acute pancreatitis (Klein et al., 2019). SAP is a disease with critical conditions, complex clinical manifestations, difficult treatment, and high mortality, and the incidence has been increasing in recent years (Pratt et al., 2018).
The course of severe acute pancreatitis is divided into three periods (early, middle, and late stages, respectively) (Jukić et al., 2018). The early stage is the onset to about 2 weeks, the first peak of death, the clinical manifestations are mainly SRS and multi-organ failure, the key to its treatment is to monitor important vital indicators, the body to stabilize the internal environment, protect the function of important organs; onset 2 to 4 weeks for the middle stage (also known as the evolutionary stage), the main clinical manifestations of necrotic fluid accumulation or peripancreatic fluid accumulation, this period is mostly aseptic necrotic foci, may also be combined with infection (Bråten et al., 2020). The clinical manifestations are mainly pancreatic and peripancreatic necrotic tissue combined with infection, deep fungal infection, systemic bacterial infection, and even serious complications such as infectious bleeding and gastrointestinal fistula. The conclusion of the correlation between CYP2C19 gene polymorphism and the clinical outcome of cerebral infarction has been controversial (Hulot et al., 2020). In the treatment of SAP, CRRT is mainly used to stop the progression of the disease by removing inflammatory mediators as soon as possible and reducing the inflammatory response. It has been shown that CRRT can significantly improve the immune hyperactivation in patients with active immune activation, while it can also partially restore the immune function in patients with suppressed immune status.
Therefore, CRRT can not only correct the water, electrolyte, and acid-base imbalance but also remove the over-activated inflammatory factors in SAP patients, regulate the immune function and re-establish the balance of the immune environment in the body, thus significantly improving the prognosis and reducing the morbidity and mortality rate of SAP patients. The treatment principle of RRT is to introduce the patient's venous blood into the filter by establishing the patient's artificial blood vessel channel, and remove small molecular substances, including electrolytes, creatinine and other substances through the principle of convection. After the convection of the replacement fluid, the blood returns to the filter. In the body of the patient, the purpose of blood purification treatment is achieved. The main principle of CRRT treatment is to achieve the purpose of blood purification by establishing artificial vascular channels for patients and using the principle of convection to remove small molecular substances in the body, such as electrolytes, creatinine and other substances. In CRRT treatment, the internal jugular vein is the first choice for artificial vascular access, followed by the femoral vein. If it is necessary, the subclavian vein can be punctured, and the venous blood of the patient can be introduced into the filter. In the body of the patient, the purpose of blood purification by extracorporeal circulation is achieved. During the treatment process, it is necessary to regularly monitor the changes in the patient's internal environment, electrolytes, coagulation function, etc., and some intervention measures can be taken to avoid the occurrence of adverse reactions. CRP is an acute protein that increases sharply in the plasma when the body is infected and tissue damage occurs, and mainly plays the role of activating complement and enhancing phagocyte phagocytosis to remove the invading pathogenic microorganisms and promote damage repair. Under normal conditions, PCT is mainly secreted by thyroid C cells, and the amount of secretion is usually <0.05 ng/mL. Under the effect of inflammation, especially bacterial infection, and sepsis, PCT can be secreted by many tissues and cells in the human body, and it is rapidly increased and reaches its peak within 12 h. The level of PCT expression in humans is stable, independent of age and gender, and is particularly sensitive to infection. The level of clinical nurses' knowledge and practice of enteral nutrition feeding intolerance needs to be improved; the current practice of prevention and management of feeding intolerance in patients after upper gastrointestinal surgery needs to be improved.
2 Related works
Evidence-based practice, as a basis for decision-making and a method of practice, closes the gap between evidence and practice (Empey et al., 2018). It breaks with the traditional, empirical model of care, emphasizes the application of the best available evidence, and is an important means of promoting professional and scientific change in clinical care practice. There are many relevant studies on FI prevention and management, according to which several mature guidelines have been developed; there are fewer such studies in China, and they lack comprehensive and in-depth exploration, and most of them are limited to critically ill patients (Martin et al., 2020). However, on the one hand, critically ill patients are characterized by severe conditions, hemodynamic instability, and application of multiple high-risk drugs; on the other hand, most of them are fed through nasogastric tubes, while most postoperative patients in the upper gastrointestinal tract use nasogastric tubes, and the two situations are far apart, which lacks the value of targeted clinical guidance for surgical nurses in China (Klein et al., 2018). Therefore, in this study, we systematically searched and evaluated the evidence related to the prevention and management of enteral nutrition FI in postoperative patients with upper gastrointestinal tract, selected the evidence appropriate to the clinical scenario, translated it into actionable, specific, and clear practice protocols for clinical nursing staff, and explored the process and model applied to the practice site (Cui et al., 2019).
Wang et al. showed that both PCT and CRP monitoring have some value in the assessment of VAP efficacy in the elderly, with PCT being more effective than CRP in predicting VAP efficacy, and the combination of the two is more helpful in further improving the accuracy of clinical efficacy prediction, and finally concluded that the combination of serum PCT and CRP after 3 d of mechanical ventilation is the best predictor of VAP efficacy in the elderly (Wang et al., 2018). Zhang et al. showed that PCT could be used to guide antibiotic discontinuation in VAP patients (Ammar et al., 2022). In the PLATO study, Xia et al. found that patients carrying the LOF allele were more likely to have cardiovascular death, myocardial infarction, and stroke at 30 days (Xia and An, 2018). A genetic subgroup study in the CHANCE study showed that the use of clopidogrel in combination with aspirin in patients with cerebral infarction within 24 h of onset was associated with lower rates of recurrent cerebral infarction and TIA in wild-type patients compared with aspirin alone, while no significant differences were found in LOF allele carriers (Li et al., 2020). The difference was not significant for LOF allele carriers (Xu et al., 2020). This suggests that the presence of the LOF allele hurts the clinical efficacy of clopidogrel in patients with acute cerebral infarction or TIA (Zhang et al., 2022). However, the conclusions drawn from the studies are not consistent.
There are many studies on the use of single indicators in the diagnosis and evaluation of VAP, and with the rise of the concept of combination, the number of studies combining different serological indicators is increasing, but there are few studies on the combination of serological indicators with scoring systems. The present study concluded that serological indicators mainly reflect the inflammatory response of the body, while the scoring system can reflect the overall physiological status of the body, and the combination of serological indicators and scoring system for the diagnosis and evaluation of VAP is a new idea, which can help to further enrich the relevant research content and obtain a research breakthrough.
3 Experimental subjects and materials
3.1 Experimental subjects
In terms of preliminary work, we collated online books and a large amount of literature to organize the influencing factors of acute pancreatitis treatment, and through the study, we analyzed the influencing factors with research value, and at the same time, we analyzed the physiological actual situation of patients with acute pancreatitis treated in our hospital to screen some potential factors of acute pancreatitis treatment, and through the collection and collation of data (Wu, et al., 2019). The therapeutic effect can be evaluated by comparing the blood amylase, leukocyte value, C-reactive protein, blood glucose, blood calcium, and other indexes before and after treatment of patients.
In this study, we are grateful for the kind help of our department and case room teachers to collect the data of patients hospitalized in the Department of Hepatobiliary, Pancreatic, and Hernia Surgery retrieved from our case room to find patients with acute pancreatitis hospitalized between October 2019 and October 2020, and record the names and hospitalization numbers of patients with acute pancreatitis one by one. In this study, after collecting the hospitalization information of patients eligible for diagnosis, and through the hospital case query system, we checked the medical records of hospitalized patients, and also obtained some information about patients during hospitalization as well as observation indexes, and after carefully reading these medical records, we screened the eligible patients and recorded the basic information of patients, examination indexes during hospitalization and other data needed for this study, and this study collected a total of 47 patients hospitalized with confirmed acute pancreatitis were randomly divided into 17 cases in the control group and 30 cases in the experimental group, 13 males and 4 females in the control group, aged 18 to 70 years, with an average of (48.33 ± 3.69) years; 21 males and 9 females in the experimental group, aged 20 to 64 years, with an average of (47.95 ± 3.62) years. By comparing the gender and age data of the two groups of patients, the differences were not significant and could be compared.
After collecting the patients' basic data, they were manually sorted and registered, after which they were entered into the computer one by one (Liu et al., 2018). We hired special quality control personnel to improve the accuracy of collecting inpatient information and to ensure the accuracy of the data, and the quality control personnel checked and corrected errors while improving the reliability of this study. The efficacy observation indexes such as blood amylase, leukocyte value, C-reactive protein, blood glucose value, and blood calcium value before and after treatment of 47 patients admitted to the hospital with acute pancreatitis who met the enrollment criteria were analyzed, and data processing and calculation analysis were performed.
The APACHE-II score and SOFA score (including admission, after 72 h of CRRT treatment) were performed on patients' admission to ICU; MCTSI score, and Marshall on admission; the duration of mechanical ventilation, duration of CRRT, days of ICU stay, and days of hospitalization and 28-day mortality were recorded and compared.
Laboratory parameters: changes in oxygenation index (P/F) and intra-abdominal pressure before CRRT and after 72 h of treatment were recorded in both groups; blood amylase before and after 72 h of CRRT treatment, as well as intra-abdominal pressure, CRP, creatinine, urea nitrogen, and calcium ions. The differences in age and sex ratio, respiratory rate, heart rate, APACHE II, SOFA score, MCTSI score, and Marshall score were not statistically significant, p > 0.05; the differences in SAP triggering factors were not statistically significant, p > 0.05, as shown in Table 1.
On admission
Group A
Group B
P
Age
53.4 ± 15.42
54.5 ± 14.42
0.257
Male /Female
14/8
12/11
0.214
Breath rate
25.97 ± 2.14
34.97 ± 3.14
0.158
Heart rate
98.11 ± 5.14
101.16 ± 4.14
0.124
APACHE II score
3.85 ± 0.14
3.94 ± 0.12
0.112
SOFA score
4.67 ± 0.14
4.85 ± 0.16
0.135
However, on the one hand, critically ill patients are characterized by serious conditions, hemodynamic instability, and application of multiple high-risk drugs; on the other hand, most of them are fed by a tube through nasogastric tubes, while most of the patients after upper gastrointestinal surgery use nasogastric tubes, and the two conditions are far apart, which lacks the value of targeted clinical guidance for surgical nurses (Shen and Lai, 2020). Therefore, this study aims to summarize the best evidence on the prevention and management of feeding intolerance in patients after upper gastrointestinal surgery using an evidence-based nursing approach and to provide a reference for the development of later protocols. Voluntarily participate in and be able to cooperate in completing various inspections.
3.2 Experimental materials and assay methods
All subjects were continuously monitored for CRP and PCT before and after mechanical ventilation treatment, and an appropriate amount (4 mL) of fasting venous blood was collected with an EP tube, and the supernatant was obtained by high-speed centrifugation (3500 rpm, 8 cm diameter, 5 min) at room temperature as the specimen to be tested. All specimens were tested immediately, and those that could not be tested immediately were stored in a refrigerator at −20 °C for testing (Zakariah et al., 2020). The immunosuppressive turbidimetric method was used to detect serum CRP levels, and the kit was purchased from Shenzhen Myra Biomedical Electronics Co. The above indexes were tested in the laboratory by the physicians of the Department of Laboratory Medicine of our hospital, and the test procedures were strictly followed following the test instructions. Recent studies and meta-analyses have found that CRRT can improve long-term renal survival, although it does not significantly improve patient survival compared with conventional hemodialysis. There is increasing evidence that high-volume hemofiltration (HVHF) does not benefit patients with sepsis-AKI, and the therapeutic dose of (20–35) ml/kg/h is still currently recommended. However, the scavenging ability of macromolecular toxins such as inflammatory mediators with the above standard dose of CRRT is very limited after all. Through meta-analysis and our recent research, it has been shown that the use of high-adsorption filters, or hybrid blood adsorption, plasma exchange and other blood purification methods are more conducive to the removal of inflammatory mediators in patients with sepsis-AKI, and significantly improve patient survival. and kidney survival rates.
CRP was detected by immunocyte turbidimeter and CRP immunocyte turbidimetric assay kit, and all assay items must be tested with reagent blanks and quality control tests, and specimens can only be tested after all of them have passed. CRP in serum reacts with goat anti-human CRP antibody to produce antigen–antibody complexes, resulting in certain turbidity, which is positively correlated with CRP concentration. The level of CRP can be detected by using an immunoturbidimetric assay to measure the turbidity after the reaction.
In the EP tube, 250 μL of the assay reagent polyethylene glycol is added (the addition of polyethylene glycol can quickly bring the reaction to the endpoint and enhance the sensitivity of the reaction); (2) distilled water (2 μL) is added dropwise, and 100 %, 50 %, 25 %, 12.5 %, and 6.25 % of the calibration stock solution are added dropwise to the tube, all 2 μL; (3) the liquid in the tube is mixed completely (4) Add 85 μL of CRP detection reagent dropwise to the tube; (5) Mix the liquid in the tube completely and treat it in a water bath (37 °C); (6) Measure the CRP level by immunocapturing turbidimeter; the normal reference range of CRP is ≤ 10 mg/L, and higher than this range is considered positive.
The purified PCT antibody was used to coat the microtiter plate, prepared as a solid phase carrier, and the specimen, standard and HRP-labeled affine were added to the microtiter wells, warmed, washed, and then color developed with the substrate, which was catalyzed by oxidase to form a blue color and converted to yellow by the action of acid, the shade of color was positively correlated with the concentration of PCT, and the absorbance (OD value) was measured at 450 nm wavelength with an enzyme standard meter (Italian ColoRectal Anastomotic Leakage (iCral) Study Group, 2020). The concentration of PCT was determined by the absorbance (OD) at 450 nm wavelength with an enzyme standard, as shown in Table 2.
Reagent
8TQ889CYLS
Manufacturer
Human STREM-1 ELISA Kit
851178
Wuhan Elite Biotechnology Co., Ltd.
PCT kit
M810067
Thermo Fisher Scientific
CRP kit
WNRA9036, WDF
BECKMAN COULTER
Blood routine kit
A9033, SLS A9009, DCL 300A G9356
SYSMEX
The use of PCT-based strategies to refine risk stratification is essential, not only for relevant treatment but also to maximize the use of healthcare resources. Studies have shown that PCT exerts toxic pro-inflammatory effects on leukocytes and cytokines, which may lead to decreased survival in patients with sepsis. A meta-analysis of 12 studies of PCT and sepsis showed a correlation between PCT and increased risk of death, with higher PCT levels associated with increased risk of death.
Patients with clinically suspected BSI should be tested with blood cultures in addition to routine testing. Performed by a clinically experienced nurse, 10 mL of venous blood is drawn and injected into special aerobic and anaerobic blood culture bottles. Specimens are collected and sent to the microbiology laboratory, where they are placed in a fully automated bacterial culture testing system and incubated until a positive result is obtained or incubated for 5 days.
A double monoclonal antibody is applied, binding to two different binding sites of calcitonin, one antibody labeled with a tracer and the other immobilized in the lumen of the reaction tube (He et al., 2019). The antigen in the specimen to be tested is added to the reaction tube coated with the monoclonal antibody for reaction. The antigen in the specimen to be tested binds to the antibody in the lumen of the reaction tube, and then the tracer-labeled monoclonal antibody is added, and after warming, an immune complex is formed and the tracer-labeled antibody binds to the lumen wall of the reaction tube, and the excess tracer is removed at the end of the reaction. The PCT in the sample is quantified by measuring the intensity of the light emitted by the tracer remaining on the wall of the tube, which is proportional to the concentration of PCT. The concentration of PCT in the sample is calculated by plotting a standard curve.
According to the patients' CYP2C19 gene test results, the patients were first randomly assigned to the medium metabolism group and the slow metabolism group, and the two groups were then randomly divided into the control group and the observation group according to the different treatment regimens. A total of 80 cases meeting the criteria were included in the study, and the number of cases in each group was 20.
3.3 Evidence-based care design
An evidence-based practice group for feeding intolerance in patients after upper gastrointestinal surgery was established with 6 members, including 1 director of the nursing department, who was the project leader and responsible for project guidance and promotion; 1 director of the nutrition department, who was responsible for nutrition-related support; 1 chief nurse, who was responsible for quality supervision and staff coordination; 1 nurse in charge of general surgery, who was responsible for nurse training and quality supervision; 1 graduate student, who was responsible for nurse training and clinical data. The definition of VAT is the same as that of VAP, but no new pulmonary infiltrates are present on portable chest radiographs. The absence of pulmonary infiltrates does not exclude the possibility that the VAT percentage may be actual VAP if computed tomography is performed. Thus, some reports of “zero VAP” may have occurred by reporting possible VAP as “ventilator-associated tracheobronchitis,” or identifying patients with intubated HAP who meet the criteria for VAP as “ventilated HAP” rather than VAP, and other possible artificially created.
A homemade clinical usability evaluation form for evidence on prevention and management of feeding intolerance was used, and the director of the nursing department, the director of the nutrition department, the head nurse of the general surgery department, and three key nurses at the practice site hospital were invited to describe the actual clinical application of the acquired evidence item by item of the evidence obtained were described (“fully applied”, “partially applied”, “not applied”) and specified. Based on the evaluation results, 8 pieces of evidence (outside the purview of nurses, lack of relevant technology and resources) were eliminated, and 14 pieces of evidence suitable for application in the practice setting were finally screened (Ahmad et al., 2018).
With the consent of the general surgery leadership, 1 investigator followed the occurrence of FI and reviewed the performance of indicators daily on a patient-by-patient basis and documented them as such. The Feeding Intolerance Prevention and Management Know-How Questionnaire and the Evidence-Based Practice Readiness Assessment Scale, supervised by the nurse manager, were distributed in paper form, and collected on-site after nurses were asked to complete them independently, with a valid return rate of 100 %, as shown in Fig. 1.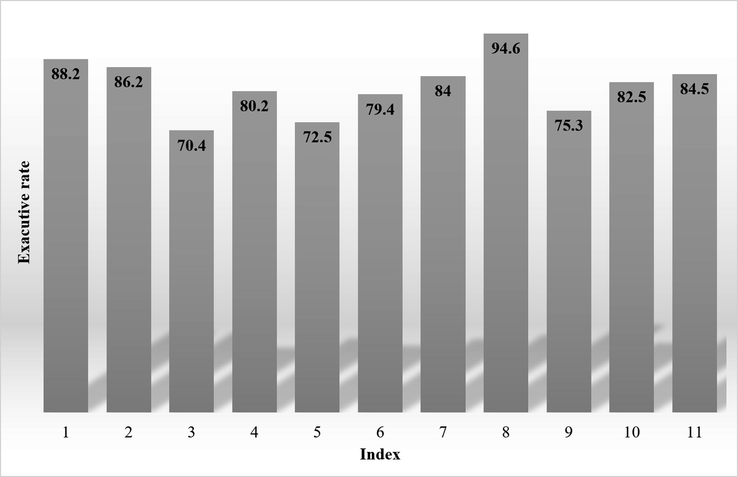
Implementation of the review indicators.
The results of the CREBNA scale survey were analyzed by nurses in the department, and the entries scoring < 4 were all entries of the evidence subscale, namely: “The application of this evidence can promote patient recovery and improve patient outcomes directly or indirectly”, “The implementation of this evidence can improve the quality of medical/nursing services”, “The evidence was assessed through a rigorous quality evaluation process”, and “The screening of the evidence incorporates the work experience and professional judgment of clinical nursing staff”. Nurses are questioning the scientific validity and applicability of the evidence (Zhang et al., 2020). Therefore, the process of evidence dissemination will focus on developing an explanation of the scientific and applicability of the evidence so that the evidence is recognized and affirmed by clinical nursing staff.
The evidence-based practice program consists primarily of action strategies, nurse training programs, and staff responsibilities. The action strategy is the corresponding countermeasures to address the barriers to evidence-based practice to promote clinical practice change; among them, the knowledge manual content is mainly the content of the evidence, knowledge of feeding intolerance assessment and management, related processes and tools, and the patient's health education manual.
4 Analysis of results
4.1 Analysis of test results
In the study, serum CRP and PCT levels were tested by professionals based on strict respect for relevant operational standards; SOFA scores were arranged to be performed by trained professionals. All examination and evaluation subjects were unaware of the content of this study to avoid subjective bias. Data collection and processing were performed by myself and trained professionals, and the data collection and entry process was performed in two groups, and the data were checked after being entered into the computer; if there was a discrepancy between the two groups of data indicating an error in the entry, it was necessary to re-collect and check the data to ensure that the data were collected and entered correctly before the study analysis.
The Receiver Operating Characteristic Curve (ROC) curve was used to analyze the value of serum CRP, PCT, and SOFA scores for the diagnosis of VAP, and the ROC curve is shown in Fig. 2. The Area Under Curve (AUC), threshold value, sensitivity, specificity, and accuracy of each index were shown in Table 3. The lowest AUC was 0.786 for CRP, with the best threshold value of 10 mg/L, followed by 0.825 for PCT, and 0.892 for SOFA. The sensitivity, specificity, and accuracy of diagnosis were 97.85 %, 96.70 %, and 97.05 %, which were higher than those of single indexes, and the differences were all significant (P < 0.05).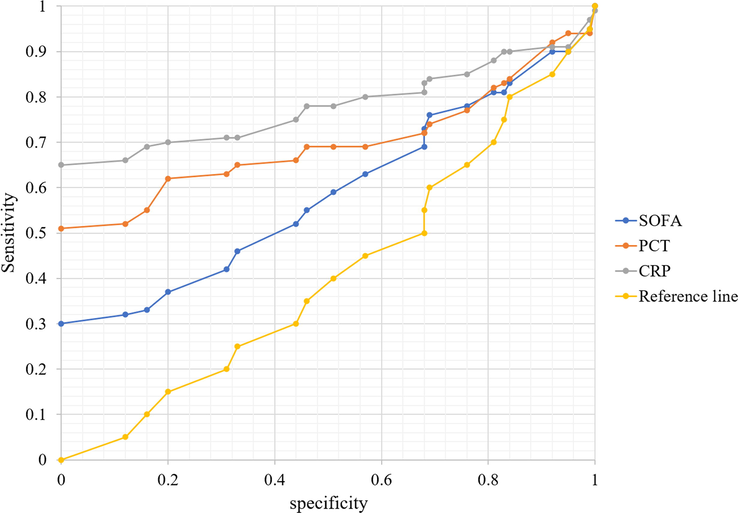
ROC curves of serum CRP, PCT, and SOFA scores for the diagnosis of VAP.
Index
AUC
Critical value
Sensitivity
Specificity
Accuracy
SOFA
0.863
12 min
0.78
0.839
0.702
CRP
0.586
12 mg/L
0.692
0.454
0.563
PCT
0.499
0.55 ng/mL
0.727
0.78
0.815
Joint
0.676
/
0.827
0.503
0.81
Before mechanical ventilation, there was no statistical difference between the serum CRP, PCT, and SOFA scores of VAP patients and non-VAP patients (P>0.05); at 48 h, 72 h and 120 h of mechanical ventilation, the serum CRP, PCT and SOFA scores of patients in the VAP group were higher than those in the non-VAP group, and the difference was statistically significant (P<0.05). Thus, serum CRP, PCT, and SOFA scores were significantly higher in VAP patients. The ROC curve was used to analyze the diagnostic value of serum CRP, PCT, and SOFA scores for VAP, and the results showed that all of them had some diagnostic value for VAP. This shows that among the three single indicators, SOFA has the highest diagnostic value for VAP, followed by serum PCT, and serum CRP has the lowest diagnostic value. In addition, this study also found that the combined application of the three indices had the highest diagnostic value for VAP, which was significantly higher than that of the single indices.
CRP is a highly sensitive inflammatory marker and the main representative of traditional inflammatory indexes. The level of CRP in the blood is low under normal conditions but increases sharply when infection, injury, or stress occurs in the body and is particularly sensitive to infection caused by bacteria. However, serum CRP can be affected by various factors and therefore lacks specificity for the diagnosis of infection. In the present study, the CRP threshold value of 10 mg/L was sensitive for VAP (80.65 %), but the specificity was poor (68.40 %), the accuracy was 72.13 %, and the AUC was only 0.786, which is consistent with the results of the study. The main reason for this is that CRP, as an acute temporal protein, is significantly elevated in patients with infectious diseases but is a non-specific acute temporal protein, and its level is significantly elevated regardless of the bodily injury, or the occurrence of acute or chronic inflammatory reactions; moreover, CRP is also affected by body stress, liver function, lipids, and age, which may result in false positives. Therefore, serum CRP alone is significantly inadequate for the diagnosis of VAP. Yes, the plasma concentration of PM type patients is higher than that of IM and EM type patients, which is consistent with the results of other studies.
The SOFA score is based on continuous variable analysis to evaluate the changes in the patient's condition, and the main features of this score are simplicity, objectivity, ease of access, and reliability; SOFA score is mainly used to evaluate the patient's organ failure status, and can be used to evaluate the condition and prognosis of ICU patients and ICU patients, and is less commonly used in VAP patients. There are few studies on the use of the SOFA score in the diagnosis of VAP, but there are more studies on the diagnosis of early sepsis by the SOFA score. In this study, the evaluation tool was selected from the EICU perspective. In this study, the SOFA score was used as a diagnostic index for VAP diagnosis, and the ROC curve analysis confirmed that the sensitivity, specificity, and accuracy of the SOFA score for VAP diagnosis were 90.32 %, 89.62 %, and 89.84 %, respectively when the critical value of SOFA score was 12, which were higher than serum CRP and PCT, and the AUC was 0.892, so it was judged that its diagnostic value for VAP was superior. This may be related to the seriousness of mechanical ventilation in ICU patients, who are mostly combined with sepsis to different degrees.
In this study, the effect of the data collected on voriconazole blood trough concentration by univariate analysis was found to be significantly affected by dose, age, and genetic metabolism type; the genetic metabolism type was found to significantly affect voriconazole blood trough concentration by optimal scaling regression; the blood concentration of PM type patients was higher than that of IM and EM type patients, which was consistent with the results of other studies. The safety of voriconazole was found to be significantly associated with CYP2C19 genotype by the exact probability method, so genetic testing can be used as a basis for guiding individualized voriconazole dosing, but unfortunately, this study did not conduct a randomized controlled trial of voriconazole gene polymorphisms and voriconazole dosing to provide a reference for the initial dosing.
However, there is some controversy regarding the value of CYP2C19 genetic test results in guiding voriconazole dosing. A systematic evaluation of the effect of CYP2C19 genotyping on voriconazole showed that patients with the PM phenotype had higher trough concentrations compared with those with the EM phenotype, and had higher treatment success rates compared with the EM phenotype, and patients with the PM There was no significant association between CYP2C19 polymorphisms and daily maintenance doses of voriconazole or adverse outcomes. Therefore, the relationship between CYP2C19 polymorphisms and daily maintenance dose needs to be confirmed by additional studies, as shown in Fig. 3.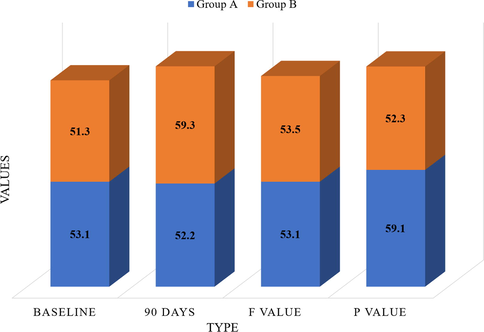
Repeated measures analysis of the separate effects of the three CYP2C19 indicators.
It indicates that patients with CYP2C19 as medium metabolism have a better effect in treating Crouse integral than patients with CYP2C19 as slow metabolism, and it is not related to whether to combine with Tonging drink treatment. It is suggested that the therapeutic effect of clopidogrel on Crouse points is different when the CYP2C19 gene is intermediate and slow metabolism, and the efficacy of intermediate metabolism patients is better.
The combination treatment with Tangbao can significantly increase HDL-C levels compared with western medicine alone, suggesting that traditional Chinese medicine may play a positive role in the development and extent of cerebrovascular diseases by regulating lipid metabolism to lower lipid levels, which may provide new ideas for future related research. Double monoclonal antibodies were used to bind to two different binding sites of procalcitonin, one antibody was labeled with a tracer, and the other was immobilized on the inner wall of the reaction lumen. However, regarding the CYP2C19 gene polymorphism, except for the Crouse score, this study did not find the effect of the difference in the medium and slow metabolism of the CYP2C19 gene on the treatment effect of each group, which may be greatly related to the small sample size. In conclusion, the therapeutic effects of Tangihanga combined with western medicine treatment on cerebral hemodynamics, carotid plaque, and lipid levels can greatly reduce the formation of intracranial and extracranial atherosclerosis, thus reducing the recurrence of stroke and related cerebral ischemic events and improving patient prognosis.
4.2 Analysis of impact results
After the application of the evidence-based practice program, the review indicators 3 and 7 were all increased from none to none, and the implementation rates were all increased by more than 80 %; the implementation rates of review indicators 1, 4, 5, 9, 10, and 11 were all increased by more than 50 %; and the implementation rates of all review indicators reached more than 80 %. After the application of the program, the review indicators 1 ∼ 5, 7, and 9 ∼ 11 was significantly improved, and the differences were statistically significant (P < 0.01), as shown in Table 4.
Review metrics
Group A
Group B
P
Implement
Not performed
Executive rate
Implement
Not performed
Executive rate
1
12
6
66.67 %
11
14
44.00 %
<0.001
2
13
11
54.17 %
11
8
57.89 %
<0.001
3
15
12
55.56 %
15
15
50.00 %
<0.001
4
14
12
53.85 %
10
6
62.50 %
<0.001
5
9
10
47.37 %
15
9
62.50 %
<0.001
6
10
14
41.67 %
9
7
56.25 %
<0.001
7
13
11
54.17 %
11
15
42.31 %
<0.001
8
7
7
50.00 %
15
11
57.69 %
<0.001
9
7
9
43.75 %
12
12
50.00 %
<0.001
10
14
15
48.28 %
15
11
57.69 %
<0.001
11
6
13
31.58 %
10
13
43.48 %
<0.001
The incidence of feeding intolerance in patients can be effectively reduced by scientific assessment and feeding intolerance management measures. In this study, the best evidence, enteral nutrition tolerance scoring scale, and enteral nutrition feeding process were incorporated into the enteral nutrition nursing process, which provided nurses with standardized assessment and operation standards, improved the accuracy of nurses' assessment and management of patient tolerance, and enhanced the quality of enteral nutrition nursing. The results of this study showed that the incidence of feeding intolerance, bloating and diarrhea in patients after the application of the protocol was significantly lower than before the application, and the time to first postoperative anal discharge and anal defecation in patients was significantly shorter than before the application of the protocol.
According to the theoretical basis discussed above, early treatment of patients with acute pancreatitis is important, and by monitoring evaluation indicators such as inflammatory factors and immune cells related to the severity of the disease and finding more meaningful monitoring criteria in clinical practice, this treatment is more targeted and can help patients improve the prognosis of acute pancreatitis. Nowadays, many experts and scholars at home and abroad have discovered many inflammatory factors through continuous exploration, including TNF-α, IL-2, IL-6, and IL-8, through which the severity of acute pancreatitis can be determined, and the changes in the condition of acute pancreatitis can be understood by observing these inflammatory factors.
By monitoring immunoglobulins and T lymphocyte subsets that are associated with acute pancreatitis, not only the immune function of the body can be identified, but also the regression of the acute pancreatitis condition can be predicted. In medicine, it can be combined with imaging examinations such as abdominal CT and MRI, which can more accurately and effectively evaluate and compare the changes in patients' conditions before and after treatment. It is also possible to evaluate and estimate the pathology of patients from different dimensions by comparing multiple testing criteria for adhesive testing and form a judgment on the prognosis of patients, and through such means, it is possible to accurately evaluate the true effect of clinical treatment with drugs.
When the critical value of SOFA score was 12 points, its diagnostic sensitivity, specificity, and accuracy for VAP reached 90.32 %, 89.62 %, and 89.84 %, respectively, which were higher than those of serum CRP and PCT, and the AUC was 0.892. The diagnostic value of VAP is better than that of serum CRP and PCT. This may be related to the severe condition of mechanically ventilated patients in the EICU, which is complicated by sepsis to varying degrees. SOFA scores are closely related to the severity and prognosis of infectious diseases. The correlation coefficient between serum PCT and SOFA score in this study was r = 0.611, p < 0.001, which means that the higher the serum PCT score, the higher the SOFA score, the more severe the organ failure, and the higher the risk of death in VAP patients. The mechanism of this relationship may be: PCT is related to bacterial endotoxin, and VAP in this study is mostly caused by gram-negative bacteria, which secrete and produce a large amount of endotoxin and increase the release of inflammatory factors, increasing serum PCT level, which in turn directly affects the bone marrow megakaryocyte system and affects blood circulation, leading to further aggravation of VAP and damage to multi-organ function; in addition, an increase in the expression level of serum PCT and other inflammatory factors also triggers an increase in serum PCT and other inflammatory factors. In addition, elevated expression levels of inflammatory factors such as serum PCT can cause cardiogenic and permeability pulmonary edema, leading to hypoxemia, decreased oxygenation index, and impaired function of multiple organs. Therefore, continuous monitoring of serum PCT and SOFA scores is more helpful in understanding the progression of VAP disease, which is the main reason serum PCT and SOFA scores are closely related to patients' prognosis and can be used to predict clinical prognosis, as shown in Fig. 4.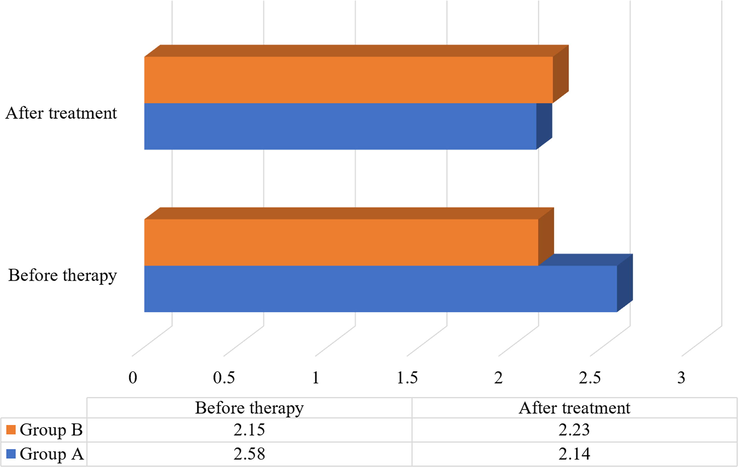
Comparison of blood calcium values between two groups of patients.
At this stage, under the action of various pathogenic factors, the cells of the body's pancreas itself are damaged to different degrees, and the production of many inflammatory factors leads to inflammatory reactions, and common inflammatory factors include mononuclear macrophages and neutrophils, etc. The body's immunity is very active at this stage, and the cytokines released at this time do not lead to acute pancreatitis. The production of cytokines can lead to pancreatic cell necrosis or apoptosis, and if the inflammatory response occurs for too long, it can also cause the formation of many inflammatory cells, which in turn can lead to the production of more inflammatory cells in the body, causing a chain cascade inflammatory response, which can eventually increase the incidence of systemic inflammatory response syndrome and multi-organ dysfunction.
At this stage, the inflammatory factor activity in the body is enhanced, and the immune function of the body tends to gradually decrease with the increasing inflammatory cell activity in the body, which makes the role of inflammatory factors in the body stronger and the immune system in the body stagnant when the body is unable to resist the invasion of foreign germs, it is easy to contract various diseases, and at this time, once the patient is infected with other diseases, it is much more difficult to control and the body is slow to recover. Therefore, it increases the morbidity and mortality rate.
As can be seen from the above, it is the increased activity of pancreatic enzymes in the body that leads to the release of a variety of inflammatory factors, and under the interaction of various inflammatory factors, many oxygen radicals begin to occur in a chain cascade of inflammatory reactions, which is the main pathogenesis of patients threatened by acute pancreatitis in the early stage; in the late stage of the disease, it is very easy to cause the migration of bacteria of intestinal origin, and many patients are infected with endotoxemia in the late stage. Many cytokines, diffuse intravascular coagulation occurs, and even more so, it can cause multi-organ failure (MOF) in patients. Therefore, in the early stage of the disease, the chain cascade inflammatory reaction should be stopped in time; in the late stage of the disease, patients should be placed in a sterile environment if necessary, to effectively control the infection and stop the production of endotoxemia, which is the most effective means of treating acute pancreatitis, especially in the treatment of severe acute pancreatitis, showing unique advantages.
5 Conclusion
SAP treatment is a comprehensive treatment involving more related specialties, even though MDT has been established in our pancreatic center for many years, it is impossible to guarantee complete homeopathic management, such as the different experience and seniority of ICU shift doctors, there is no uniform standard for each treatment of patients with SAP, and sometimes it depends more on personal experience and habits, which all affect the comparability between patients to some extent. PCT is low in the healthy Elevated PCT levels are a key laboratory indicator of acute infection. When the body is exposed to bacterial infection, the expression of PCT levels is upregulated in response to inflammatory stimuli, and its levels in the serum increase rapidly. PCT has a long half-life in the blood and is a useful adjunctive test for screening bacterial infections. PCT levels are less elevated in localized bacterial infections and severe viral infections. It indicates that patients with CYP2C19 as a medium metabolizer are better treated with Crouse integral than patients with CYP2C19 as a slow metabolizer, and it is not related to whether to combine with Tonging drink treatment. It is suggested that the therapeutic effect of clopidogrel on Crouse points differs when the cYP2C19 gene is intermediate and slow metabolism, and the efficacy is better in intermediate metabolism patients. In this study, there was no significant correlation between serum CRP and SOFA scores, although it is consistent with the findings of many studies so far, and this study suggests that this is mainly related to the differences in the types of pathogenic bacteria and severity of infection in patients in different studies, and the specific reasons for this remain to be confirmed by further studies. In the future, we will conduct further research and analysis on this basis.
Acknowledgement
The authors are thankful to the higher authorities for the facilities provided.
Data Availability Statement
The data used to support the findings of this study are available from the corresponding author upon request.
Funding Statement
The research was funded by the key project plan of medical science research of Hebei provincial health and Family Planning Commission in 2016 topic: application of evidence-based nursing in prevention of continuous blood purification and treatment of coagulation during cardiopulmonary bypass Project No.: 20160480.
Declaration of Competing Interest
The authors declare that they have no known competing financial interests or personal relationships that could have appeared to influence the work reported in this paper.
References
- Nurses and internet health-related information: review on access and utility. Clujul Med.. 2018 Jul;91(3):266-273.
- [CrossRef] [Google Scholar]
- The role of lung ultrasound in procalcitonin-guided antibiotic discontinuation in ventilator-associated pneumonia. Indian J Anaesth.. 2022 Jun;66(6):431-435.
- [CrossRef] [Google Scholar]
- Impact of CYP2C19 genotype on sertraline exposure in 1200 Scandinavian patients. Neuropsychopharmacology.. 2020;45(3):570-576.
- [CrossRef] [Google Scholar]
- Prognostic significance of PCT and CRP evaluation for adult ICU patients with sepsis and septic shock: retrospective analysis of 59 cases. The. J. Int. Med. Res.. 2019;47(4):1573-1579.
- [CrossRef] [Google Scholar]
- Multisite investigation of strategies for the implementation of CYP2C19 genotype-guided antiplatelet therapy. Clin. Pharmacol. Ther.. 2018;104(4):664-674.
- [CrossRef] [Google Scholar]
- Correlation between serum PCT, IL-6 and CRP levels and pulmonary ventilation function in AECOPD patients. J. Hainan Med. Univ.. 2019;25(6):47-50.
- [Google Scholar]
- Routine CYP2C19 Genotyping to Adjust Thienopyridine Treatment After Primary PCI for STEMI: Results of the GIANT Study. Cardiovasc. Interv.. 2020;13(5):621-630.
- [CrossRef] [Google Scholar]
- Italian ColoRectal Anastomotic Leakage (iCral) Study Group. 2020. Anastomotic leakage after elective colorectal surgery: a prospective multicentre observational study on use of the Dutch leakage score, serum procalcitonin and serum C-reactive protein for diagnosis. BJS Open. 4(3), 499–507. https://doi.org/10.1002/bjs5.50269.
- Clinical outcomes of CYP2C19 genotype-guided antiplatelet therapy: existing evidence and future directions. Pharmacogenomics. 2018;19(13):1039-1046.
- [CrossRef] [Google Scholar]
- Clinical utility of CYP2C19 Genotyping to guide antiplatelet therapy in patients with an acute coronary syndrome or undergoing percutaneous coronary intervention. Arterioscler. Thromb. Vasc. Biol.. 2019;39(4):647-652.
- [CrossRef] [Google Scholar]
- Serum amyloid a is a biomarker of severe coronavirus disease and poor prognosis. J. Infect.. 2020;80(6):646-655.
- [CrossRef] [Google Scholar]
- Detection of serum procalcitonin and hypersensitive C-reactive protein in patients with pneumonia and sepsis. J. Biol. Regul. Homeost. Agents.. 2018;32(5):1165-1169.
- [Google Scholar]
- Frequency and clinical outcomes of CYP2C19 genotype-guided escalation and de-escalation of antiplatelet therapy in a real-world clinical setting. Genet. Med.. 2020;22(1):160-169.
- [CrossRef] [Google Scholar]
- Effect of CYP2C19 genotype on ischemic outcomes during oral P2Y12 inhibitor therapy. JACC Cardiovasc. Int.. 2021;14(7):739-750.
- [CrossRef] [Google Scholar]
- Recommendations for clinical CYP2C19 Genotyping allele selection. J. Mol. Diagn.. 2018;20(3):269-276.
- [CrossRef] [Google Scholar]
- Diagnostic Value of sCD163 Combined with PCT and HS-CRP in Patients with Gynecological Malignant Tumors and Fever. J. Coll. Physicians Surg. Pak.. 2020;30(10):1053-1057.
- [CrossRef] [Google Scholar]
- Dynamic changes and diagnostic and prognostic significance of serum PCT, hs-CRP and s-100 protein in central nervous system infection. Exp. Ther. Med.. 2018;16(6):5156-5160.
- [CrossRef] [Google Scholar]
- The predictive value of joint detection of serum amyloid protein A, PCT, and Hs-CRP in the diagnosis and efficacy of neonatal septicemia. Eur. Rev. Med. Pharmacol. Sci.. 2019;23(13):5904-5911.
- [CrossRef] [Google Scholar]
- Serum folic acid, PCT, CRP and ESR detection as biomarker in differentiation ulcerative colitis activity. Pteridines. 2018;29(1):179-186.
- [CrossRef] [Google Scholar]
- Curative effects of vancomycin and cefotaxime combined with gamma globulin respectively in neonatal septicemia and their influences on PCT, CRP and hs-CRP. Eur. Rev. Med. Pharmacol. Sci.. 2020;24(8):4486-4494.
- [CrossRef] [Google Scholar]
- Is Procalcitonin more superior to hs-CRP in the diagnosis of infection in diabetic foot ulcer? Malays. J. Pathol.. 2020;42(1):77-84.
- [Google Scholar]
- Diagnostic Value of ROC Curve Evaluating Serum Related Indexes for Bloodstream Infection in Patients with Hematopathy. Zhongguo Shi Yan Xue Ye Xue Za Zhi.. 2020;28(5):1746-1749.
- [CrossRef] [Google Scholar]
- Effects of Gegen Qinlian Decoction combined with Chinese herbal hot package on the expression of PCT, CRP and IL-6 in patients with acute gastroenteritis. Cell. Mol. Biol.. 2022;68(2):189-196.
- [CrossRef] [Google Scholar]




